“WHERE THERE IS HOPE, THERE IS LIFE: AN ALTERNATIVE TO PHYSICIAN-ASSISTED SUICIDE, CONSIDERING CHINESE AND WESTERN PERSPECTIVES ON LIVING THROUGH TERMINAL ILLNESS IN CHINA”
Author: Philip Hung-wong Chiu, Hons. B.Sc. (Psychology) with 1st Class Honor (McGill); M.D.(Queen’s, Canada), F.R.C.S.(C), F.A.C.O.G. ; M.B.P.A. (UC Irvine); M.Div. & Th.M. (Golden Gate Baptist Theological Seminary, now Gateway); M.A. (Pastoral Care and Counseling) & Ph.D. (Psychology & Practical Theology) from Claremont School of Theology. See Facebook and Youtube.com under Philip H Chiu.
Abstract:
What is it that prompts the tormented terminally ill to choose life, instead of killing themselves? The thesis here presented is that hope can provide them a positive attitude to remain engaged in life. Many of the peasants and “urban poor” in China are in a dilemma when afflicted with a terminal illness: on the one hand, they can ill afford even pain relief; and on the other, their requests for Physician Assisted Suicide cannot be honored because it is still illegal in China. Interdisciplinary literature review suggests that hope appears to be uniquely suited to deal with the existential concerns of these people. Field work in Southern China also lends support to the thesis.
Chapter One outlines the challenges of providing health care in China. Using interviews conducted by the author, Chapter Two describes some of the ways people live through terminal illness in China, and how they manage to find meaning and hope in their cultural beliefs, strengths and values. Chapter Three explores, from the perspective of the Western philosophical tradition, the question that some of these interviewees are asking: What is my meaning of life? This brings into discussion the views of both the “True world” and “Continental” philosophers.
An interdisciplinary discussion of hope (Chapter Four) suggests that four dimensions of hope, the first virtue in life followed by will, may be uniquely equipped in addressing the needs of the terminally ill. Chapter Five examines the question “Is Fostering Hope Justified in the Terminally Ill?” ethically, existentially, and scientifically. Chapter Six outlines different ways as to how hopefulness can be fostered by caregivers, with due respect given to the unique cultural setting of the afflicted. In conclusion, it appears that when the terminally ill have hope, they remain engaged in life, making Physician Assisted Suicide less of an issue. It should be noted that the author’s social location as a Southern Baptist minister, an endorsed chaplain, and a retired physician trained in Western medicine may have lent predispositions and biases to the interpretation of literature and research interviews.
This book outlines a strategic intervention in pastoral care that focuses on care for the terminally ill and their families (essentially in Chapter 6). For this reason, this book may be of interest not only to spiritual caregivers, but also to students of the social sciences and healthcare personnel such as nurses and doctors. I do hope that my contribution can also serve as a catalyst to continuing dialogues between health care policy makers, spiritual caregivers and the public. Together, we can offer the best end-of-life care to all concerned.
Introduction
During my 15 months of service as a spiritual caregiver[1] and counselor in a major hospital in China, I was saddened by the intractable pain and suffering[2] of a number of terminally ill[3] patients who requested Physician Assisted Suicide (PAS) because they could not afford the expensive palliative care. They were in a dilemma. Some of them had spent all their life savings on medical care. Thus, many were already heavily into debts, which had created considerable financial burden on their families. To stay the course would have meant suffering the indignity of wasting away under the ravages of their disease, and incurring further debts and burdens on their families. They wanted to die, but were unsure about the best way to end their lives with dignity. Knowing that I am a physician as well as a spiritual caregiver, they asked me about PAS, thinking that somehow I could advise them or even help them with this “good death” (an le si in Chinese, or “mercy killing” as PAS is known in China). I was in a dilemma too. First, PAS is still illegal in China. Second, my Christian faith and my commitment to the Hippocratic Oath[4] would not allow me to do such a thing, even though I empathized with their suffering. Suicide by any means raises serious issues: ethical, socio-cultural, politico-medico-legal as well as spiritual and relational. I propose another option: fostering hope as an interventional strategy, based on the thesis: where there is hope,[5] there is life.[6]
The Core Problem in its Relevant Contexts
China is a country in transition. Her entry into the 21st century has been marked by astonishing economic growth and prosperity, but not without cost. There is now a wider disparity between the rich and the poor. China’s transition from state-owned businesses to free enterprise has left many of her citizens without adequate healthcare, which used to be provided by the state. When confronted with a terminal illness, the poor often cannot afford the expensive care and pain relief at the hospital. Neither do they have any kind of hospice program to alleviate their suffering and provide them support at home. No wonder more and more of these patients are asking about PAS. Unlike some countries in the West (such as the Netherlands and Belgium), China has not embraced this concept as yet. For me, a retired Chinese-born American physician and a Christian minister and chaplain, my heart goes out to these patients. At the same time, I often wonder if I can truly understand the Chinese perspective on suffering and “good death.” What would it mean to the terminally ill and their families as well as their caregivers to live through this ordeal in China? What sustains them, and what are their reasons for living? How can chaplains and other caregivers best support them?
Thesis and Flow of Argument
When I see these terminally ill patients suffering from unimaginable pain physically, emotionally and financially, I ask myself the same question many times: What is it that prompts many of these tormented people to choose life, instead of killing themselves? It is the same question that Viktor Frankl asked while confined in the Auschwitz concentration camp. He found the answer in “will to meaning,” which sustains the lives of his fellow inmates.[7] Building on this notion, I submit that hope may provide the terminally ill with a positive attitude to remain engaged in life even in the darkest of times. Hope allows one to project into the future for positive meaning in the present. I submit that when the terminally ill seriously consider suicide, hope may deter them from such an act. In the words of James Cone, the theologian, “Without hope, you die.” [8]
I argue that not only can hope rest in meaning[9] as an experiential process, it can also rest in: love and support[10] as a relational process; in faith and trust[11] as a spiritual or transcendent process; and in choosing realizable goals and attaining them[12] as a rational process. These dimensions of hope[13] appear to be uniquely suited to deal with the existential concerns that are commonly found in the terminally ill, namely meaninglessness, isolation, groundlessness, and death.[14] Hope has also been argued to be the first virtue (or human strength) that develops in the human life cycle.[15] To the extent that strengths build upon prior strengths, this means that hope is the basis for all other strengths.
Hope, as vision, also takes on differently colored lenses according to varying cultural and communal contexts. Chinese and Western perspectives on meaning and hope bring to light assumptions and presuppositions in both perspectives and each enriches the other. It is my fervent hope that the terminally ill, Chinese or otherwise, will benefit from this exchange of ideas and have access to more options to help them cope with their suffering and achieve a quality of life that they perceive as satisfying.[16]
Overall, this dissertation argues the following points: (1) building on Viktor Frankl’s will to meaning, and the unique characteristics of hope (including its widespread significance, spiritual implications, and relational and rational nature), I submit that hope can provide the terminally ill with a positive attitude to remain engaged in life even in the darkest of times, making suicide less of an issue; (2) hope is uniquely equipped to deal with the existential concerns of the terminally ill, resting in meaningful experiences, trust and love, faith and spirituality as well as rational thoughts and actions; (3) hope is not something that can be given to or imposed on the cared-for, but an attitude or virtue that can be fostered in and reinforced by the cared-for through practice; (4) the one-caring can infuse a sense of hopefulness into the caring environment through an unwavering commitment to caring for the other person; and (5) fostering hope needs to take into consideration the cultural and communal settings of the cared-for.
Research Methods
The primary method used in this research is literature review and critical analysis. Research interviews were conducted to supplement this literature analysis. The research question I had in mind was two-fold: (1) when the poor with terminal illness in China cannot afford their medical care and get adequate pain relief, what is life like for them and their family caregivers, and (2) what role can be played by the family and professional caregivers to meet some of their needs? In relation to both questions, I was especially interested in the value of hope. My field work in China consisted of research interviews that investigated the experience of living through terminal illness in China and identified, through literature review, the means of relevant spiritual care for suffering, for finding life’s meaning, for existential concerns, and for fostering hope.
Through personal contacts and professional relationships with patients, physicians, spiritual caregivers and counselors in Southern China, the author interviewed twenty-three individuals in China during the period October 2007 to January 2008. Fifteen of them were afflicted with terminal illness, five were related family members, and three were spiritual counselors (one Taoist priest, one Buddhist physician, and one Imam). In these interviews, only open-ended questions were asked in order to encourage the interviewees to tell their stories. Closed questions that would elicit only “yes” or “no” answers were avoided. Any reference to hope by the interviewer was implicit. Generally, three questions were posed: (1) Can you describe your understanding of suffering? What does it mean to you? (2) What would be your experience with this illness that has affected you (or your family)? (3) How would you (or your family) view life and death when dealing with this illness? Special attention was paid to causal factors, intervening factors and contextual factors that affect suffering, and to the coping strategies as well as consequences. After each interview, short notes were written within an hour, and a summary of each interview was typed out within twenty-four hours. Statements from each interviewee were quoted as faithfully as possible (see Appendix). Some of the stories and comments I heard in this field work are used throughout the dissertation to illustrate, where appropriate, pertinent points brought out by the literature on meaning of life and hope, bringing together Chinese and Western resources on helping these people live through terminal illness.
It should be pointed out at the onset that these research interviews were not conducted according to formal empirical standards. My argument regarding hope in the terminally ill remains untested empirically. Such research work in the future might better establish its validity. The rigorous standards of empirical research were not employed for the interviews, because the Chinese Government is resistant to any research project seen as religious. Officially, religious organizations in China today must be Government-recognized and approved. The three state-endorsed religious organizations are the Chinese Patriotic Catholic Association, the Three-Self Patriotic Movement for Protestants,[17] and the Chinese Patriotic Islamic Association. Buddhism and Taoism are the two other religions officially recognized by the state. Confucianism is considered as a philosophy and not a religion in China.
References:
[1] Spiritual care is defined here as care that encourages and supports the cared-for’s own reflections on experience, search for meaning and purpose, and development of inner resources for the spiritual journey.
[2] Suffering is defined here as distress that arises from an individual’s perception of pain.
[3] Terminal illness is defined here as an active and progressive disease that cannot be cured or adequately treated and which is expected to lead to the eventual death of the patient.
[4] The Hippocratic Oath I follow as a physician says in part, “I will not give a lethal drug to anyone if I am asked, nor will I advise such a plan.” The National Institutes of Health’s History of Medicine Division provides a full text of the Hippocratic Oath on its website. http://www.nlm.nih.gov/hmd/greek/greek_oath. html (accessed May 20, 2008).
[5] Hope is defined by Erik H. Erikson as “an attitude, an enduring belief in the attainability of fervent wishes” in “Human Strength and the Cycle of Generation,” Insight and Responsibility (New York: W. W. Norton, 1964), 118.
[6] This phrase first appeared, as far as I know, in the title of an article by Robert L. Richardson, “Where There is Hope, There is Life: Toward a Biology of Hope,” Journal of Pastoral Care 54, no. 1 (Spring 2000), 75-83. Life refers to the quality that distinguishes a vital and functional being from a dead body (Merriam-Webster Dictionary).
[7] Viktor Frankl, Man’s Search for Meaning: An Introduction to Logotherapy, rev. and trans. Ilse Lasch, rev. and enl. ed. (Boston: Beacon Press, 1962), 113.
[8] Quoted in an article in the March 19, 2008 edition of Newsweek. http:// www.Newsweek/ Washingtonpost.com (accessed May 20, 2008).
[9] Frankl, Man’s Search for Meaning,105.
[10] Gabriel Marcel, as related by Jean Nowotny, “Despair and the Object of Hope,” in The Sources of Hope, ed. Ross Fitzgerald (Rushcutters Bay, Australia: Pergamon Press, 1979), 66.
[11] Paul W. Pruyser, Between Belief and Unbelief (New York: Harper & Row, 1974), 198-213.
[12] Erik H. Erikson, “Human Strength and the Cycle of Generations,” Insight and Responsibility (New York: W. W. Norton, 1964), 117.
[13] Carol J. Farran, Kaye A. Herth, and Judith M. Popovich, Hope and Hopelessness: Critical Clinical Concepts (Thousand Oaks, CA: Sage Publications, 1995), 6.
[14] Irvin Yalom, Existential Psychotherapy (New York: Basic Books, 1980), 8.
[15] Erikson, “Human Strength and the Cycle of Generations,” 115.
[16] Quality of life is defined by the Center for Disease Control and Prevention (Atlanta, Georgia) as an overall sense of well-being with a strong relation to a person’s health perceptions and ability to function.
[17] This Movement is characterized by self-governance, self-support (without financial dependence on foreigners) and self-propagation.
TABLE OF CONTENTS
Chapter 1. Health Care in China
Overview
Economic and Social Change
Demographic Change
Medical Need among the Elderly
China’s Strategy in Managing Transition
Evolution of Health Care in China
The Period Between 1949 and l965
The Period of the Great Cultural Revolution 1965 – 1978
Problems of the Traditional Health Care System
Health Care Reform (from 1980s)
Emergence of Basic Health Insurance (urban)
Reform in Cooperative Health Care (rural)
Current Management of Health Care
Fiscal Decentralization
Financial Responsibility System
Government’s Price Reform
Evaluation of Health Care Reform since 1978
Overall functioning of China’s health care delivery system
Disparities between China’s Rural and Urban Areas
Equity in Accessing China’s Health Care
Summary
Chapter 2. Living Through Terminal Illness in China
Living Through Terminal Illness in China
Chinese Perspectives on Suffering
Chinese Cultural Beliefs
Uncontrollability
Ubiquity of Change
Fatalism
Dualism
Collectivism
Utility of Efforts
Strengths and Virtues in Coping
Chinese Perspectives on Life and Meaning of Life
Chinese Perspectives on “Good Death”
Chapter 3. Western Philosophical Perspectives on Meaning of Life
Western Philosophical Perspectives on Meaning of Life
True-World Philosophy
Continental Philosophy
Quality of Life
Search for Existential Meaning
Critique and Discussion
Implications for the Terminally Ill
Chapter 4. Hope
What is Hope?
The Earliest Virtue
Development of Hope
Chinese Perspectives on Hope
Western Perspectives on Hope
Four Dimensions of Hope
Christian Theology of Hope
Grounding in Scripture
Contemporary Theology of Hope
Critique
Pastoral Theology of Hope
Summary and Discussion
Chapter 5. Is Fostering Hope Justified in the Terminally Ill?
Ethical Consideration
Existential Consideration
Meaninglessness and Hopefulness
Isolation and Hopefulness
Groundlessness and Hopefulness
Death and Hopefulness
Research Consideration
Biology of Hope
Chapter 6. Fostering Hope in the Terminally Ill
General Considerations
Cultural Considerations
Role of Physicians
Role of Hospice Programs
Role of Pastoral Caregivers
Where there is Hope, there is Life
Acknowledgments
The author wishes to acknowledge the expertise provided by Professor Kathleen Greider, Professor Ellen Marshall, Professor Samuel Lee from Claremont School of Theology (CST) in the preparation of these manuscripts. In addition, without the scholarships provided by Professor William Clements and the Chinese Baptist Church of Orange County, this dissertation would not have been possible. Throughout these many years of study, my wife Rosangela has stood by my side, providing every possible help that I need. To all these wonderful people I express my sincere gratitude.


CHAPTER 1: Health Care in China
Overvie China is in transition. She is in transition from a command economy to a market economy; from a rural society to an urbanized and industrialized society; and from isolation to welcoming the whole world in the 2008 Summer Olympics in Beijing. Communication is rapidly expanding within the country and with the rest of the world. Together with the other transitions, the age structure and medical needs of her citizens are also in transition. While China is now the fastest growing economy in the world, her torrid economic growth has been uneven, leading to a wider gap between the rich and the poor. Such discrepancy can be reflected in the health care sector today.
According to official statistics, China is still a largely rural society. However, over the past 20 years the proportion categorized as urban has grown sharply. In the year 2000, 458 million people were registered as permanent residents of urban areas, or 36.2% of the total population (see Table 1).
Table 1: Trend in urban population growth, 1980-2000
| Year | Total population in millions | Urban population in millions | Proportion in percentage |
| 1980 | 987 | 191 | 19.4 |
| 1985 | 1059 | 251 | 23.7 |
| 1990 | 1143 | 302 | 26.4 |
| 1995 | 1211 | 352 | 29.0 |
| 2000 | 1266 | 458 | 36.2 |
In 1980, there were 223 cities, of which 15 had more than a million people.
Twenty years later there were 663 cities, of which 41 were bigger than a million (see Table 2).[1] These changes are due to a combination of in-migration and the re-classification of areas from rural to urban.
Table 2: Number of cities by size of non-agricultural population
| City size | 1980 | 1991 | 2000 |
| 2 million + | 7 | 9 | 14 |
| 1-2 million | 8 | 22 | 27 |
| 0.5-1.0 million | 30 | 30 | 53 |
| 0.2-0.5 million | 72 | 121 | 218 |
| less than 0.2 million | 106 | 297 | 352 |
| Total | 223 | 479 | 663 |
Classification of a household as urban or rural greatly affects its entitlements.
Registration status has important implications for a household’s ability to obtain employment and secure social benefits. Officially sanctioned rural-to-urban migration requires a formal household registration or hukou transfer from agricultural to non-agricultural status. Without this registration, these migrants would have difficulty securing employment and health care benefits in the urban area. Rural-to-urban migrants now constitute an important, but unknown, proportion of urban residents.
Economic and Social Changes
China has experienced more than 20 years of sustained economic growth which has led to rapid rises in average annual disposable income per capita, rising from CNY343 (Chinese Yuan) in 1978 to CNY6,280 (under USD1,000) in 2000.[2] This has been associated with changes in patterns of consumption. One sign of the pace of change is the increase in the number of color television sets per 100 households in urban areas from 17.2 to 116.6 between 1985 and 2000. Even the poorest 10 per cent of urban households had 99 sets per 100 households. Television reached 93.7% of China’s population in 2000. This provides an indication of the rapid growth in communication that has accompanied economic growth. Many goods and services, including health-related ones, are now advertised on television, radio and in print media. This has influenced popular expectations.
However, economic growth has not been distributed evenly. The eastern parts of the country have developed much more quickly than the west. In 2000, the Gross Domestic Product (GDP) per capita ranged from CNY2,662 in Guizhou (in south-western China) to CNY22,460 in Beijing.[3] In addition, there are substantial differences in the economic well-being of households within each locality. In 2000 the poorest 10% of urban households had an annual income of CNY2,678 per capita, compared with CNY13,390 for the richest 10%.[4] These substantial inequalities have a number of effects. On the one hand, the patterns of consumption of the richer groups influence overall expectations of life styles.
In recent years, a group of urban poor has emerged, which includes the unemployed, the under-employed, the disabled, the retirees, and those who were laid off. The growing economic inequality is largely associated with increasing diversity in types of employment. In 1980, most urban jobs were in state- or collectively-owned enterprises. In 2000, employment in the first two categories had fallen, while a larger number of people (12.7 million compared to 4.9 million in 1995) worked for privately-owned companies. Over 20 million people were self-employed (see Table 3 below):
Table 3: Number of employed people (in millions) in urban areas by type of employee
1980 1985 1990 1995 2000
| State-owned enterprises SOEs | 80.2 | 89.9 | 103.5 | 112.6 | 81.0 |
| Collectively-owned enterprises Collectively-owned enterprises | 24.3 | 33.2 | 35.5 | 31.5 | 15.0 |
| Privately owned companies | — | — | 0.6 | 4.9 | 12.7 |
| Self-employed | 0.8 | 4.5 | 6.1 | 15.6 | 21.4 |
In the mid-1980s, the government introduced labor contract system to replace the previous guarantees of “work until retirement” in state-owned enterprises (SOEs), making it possible to lay off workers when these SOEs became unprofitable. Thus, even though the registered unemployment rate in urban areas has been consistently quoted as 3.1% since 1997 according to national statistics,[6] the real unemployment rate was found to be 6.99%
in 1999, when the number of laid-off persons was taken into account.[7] Even though women did not make up a disproportionate share of the total numbers of laid-off, their unemployment rate, as related to their total employment, was higher than men, since they made up less than half of the workforce. These laid-off workers, together with the other unemployed and disabled, constitute the urban “poor and vulnerable” at the very bottom of the social scale.[8]
The government has defined minimum living standards for urban areas, below which people are entitled to financial support. According to a survey by the Ministry of Civil Affairs, which oversees the “poor and vulnerable,” around 14 million urban residents had an income below the local poverty line in 2000, varying from CNY1,680 to CNY3,828 on average per person according to the city. Poverty lines reflect differences in the cost of living and in the capacity of city governments to pay income supplements. Also, poverty lines for residents of “rural” counties within municipal boundaries are actually much lower than the average quoted. In addition, many more people have incomes just above the poverty line. This suggests that quite large numbers of people are poor or at risk of impoverishment. This has important implications for health care.
Demographic Change
The age structure of China’s population is also changing rapidly. An active family planning policy and factors associated with economic and social development, together with rising average life expectancy have led to a fall in the proportion of young people (below the age of 15 years) and a rise in the proportion of elderly (65 and over). The proportion over 65 years grew from 3.6% in 1964 to 7.0% in 2000 (See Table 4 below). The proportion over 75 years old more than doubled from 0.8% in 1964 to 2.2% in 2000. This aging of the population is expected to continue and have a significant impact on the future health care system in China.
Table 4: Age structure of China from 1964 to 2000 [9]
| Age (in years) | 1964 (%) | 1982 (%) | 1990 (%) | 2000 (%) |
| 0-14 | 40.7 | 33.6 | 27.7 | 22.9 |
| 15-64 | 55.7 | 61.5 | 66.7 | 70.1 |
| 65+ | 3.6 | 4.9 | 5.6 | 7.0 |
| 75+ | 0.8 | 1.4 | 1.7 | 2.2 |
Medical Need among the Elderly
Medical need has been defined as the existence of ill-health for which an effective treatment is available.[10] The extent of medical need is a measure of the physiological and psychological well-being of individuals; their expectations of what constitutes well-being; the availability of effective interventions; and the social arrangements that determine the roles of households and health providers in caring for the sick. According to this definition, medical need is determined by the burden of sickness and the social consensus about the kinds of support sick individuals require. Both determinants are changing in China, it seems.
The aged account for a substantial share of medical care costs in urban China. Data from advanced market economies suggest that average medical care costs rise rapidly with age.[11] Those over 75 years old have a particularly great need for expensive health care.
One reason for this is because of the nature of the diseases affecting the elderly, who have a prevalence of cardiovascular diseases and cancer, as well as chronic illnesses.[12] Another reason for the high cost is because of changes to family structures which have made family members less able and less willing to care for their sick relatives at home.[13] The lack of affordable medical support for the aged puts a heavy burden on family caregivers, particularly women, who stay home while men go out to work.
China’s Strategy in Managing Transition
China’s strategy in managing her economic transition is highly decentralized.[14] On the revenue side, each level of government can collect taxes. It retains most of the taxes and transfers some to higher levels according to complex and changing rules. In addition, county or city governments may also have substantial sources of revenue in addition to taxes. Many own enterprises that pay profits or management fees. Some also own land and collect ground rent. With this revenue, the local governments can have a great deal of autonomy in deciding how to use it. They can use this “extra-budgetary revenue” as they wish. Under this fiscal decentralization, local governments can, since the early 1980s, decide how much money or how big a grant to allocate to support health care facilities in their localities. The Ministry of Health has delegated this authority to them while maintaining only a supervisory relationship with the levels of government below it.
This fiscal decentralization has had two important consequences. It has led to growing differences in the resources available to local governments: some have very substantial revenues and others can barely pay salaries. It has also given local governments a lot of control over their own resources, and has limited the capacity of higher levels of government to do so.
It is important to note that the Chinese government is organized in a number of vertical structures that extend from national to local administrative levels. Each level of local government more or less replicates the structure at national level. For instance, each level of district/county and higher local government has a health department which is answerable to the government at the same level and to the health department of the next higher level. At each level, there are hospitals, preventive services, medical institutions, and health training schools, a majority of which are directly supervised by the corresponding health department. Such organization into parallel vertical channels has advantages and disadvantages. It has established close accountability, resulting in very effective preventive health programs at the grass roots. Furthermore, the close accountability makes it less likely for government health facilities to treat their own healthcare providers with favoritism. However, this system ends up having numerous commissions, ministries, and bureaus/agencies that have health-related mandates for planning, service provision, regulation and accountability, as well as financing.
In Table 5 below, it can be seen how this high degree of bureaucracy makes it difficult to formulate coherent healthcare development strategies and creates a nightmare in coordination. It is the Ministry of Civil Affairs and the civil affairs departments at provincial and lower levels that provide the safety nets for the poor and vulnerable.
Table 5: Government Organizations with an Influence on Health Care for the Poor and the Vulnerable [15]
For Planning – The State Development Planning Commission oversees the formulation of health care policies. It is also responsible for the implementation of five-year regional health plans.
For Service Provision, Finance, Regulation and Accountability – The Ministry of Health, under the authority of the State Council (which also oversees other reforms beside health reform, including economic and social reforms), provides overall leadership to the health sector. It is responsible for the performance of health institutions; provides annual grants to government health facilities (including public health); contributes to local health insurance schemes for government employees; and regulates all government health facilities as well as private healthcare providers.
For Regulation and Accountability – other bureau and ministries:
- The Price Bureau of State Development Planning Commission sets prices for health services and health-related commodities. There are similar price bureaus at the provincial, county, and municipal levels.
- The Ministry of Personnel manages civil servants as well as skilled workers in public employment.
- The Ministry of Labor and Social Security manages semi-skilled and unskilled laborers in public employment. This office was set up in 1997 to develop the Social Security system in China. It also sets up the Urban Basic Health Insurance.
- The State Drug Administrative Bureau was set up to develop drug-related regulations, approve the use of new drugs, and monitor the effective and safe use of all drugs in China. Initially the Bureau was established within the Ministry of Health, but has now become an independent government agency. At the provincial and lower levels, respective bureaus responsible for drug administration were also set up to carry out the same functions.
For Financing – beside Ministry of Health and Ministry of Labor and Social Security:
- The Ministry of Civil Affairs and the civil affairs departments at provincial and lower levels provide the safety nets for the poor and vulnerable.
So far, we have seen how China manages the health care of her people through a highly decentralized fiscal policy as well as a highly bureaucratic system of government. There are pros and cons in each of these as mentioned earlier. How successful have they been in responding to the health care needs of the Chinese people? Let us now take a look at the evolution of health care in modern China from the founding of the People’s Republic to the present time.
Evolution of Health Care in China
The history of health care in modern China can be generally divided into three periods: (1) from the founding of the People’s Republic in 1949 to the eve of the Great Cultural Revolution in 1965; (2) the years in which the Great Cultural Revolution was taking place (1966-77); and (3) from the beginning of the economic reform in 1978 to the present.
The Period Between 1949 and l965
When the People’s Republic of China was established by the Chinese Communist Party in 1949, the country had inherited a poorly developed health sector.[16] The major medical care providers were Traditional Chinese Medicine (TCM) practitioners who used a combination of herbal medicine, acupuncture and other traditional methods to treat patients. The relatively small number of doctors of Western medicine worked mainly in the urban hospitals.
In 1951 the First National Health Conferences sponsored by the State Council of the new government was held and the following health policies were announced:[17]
- Medicine must serve the working people (workers, peasants and soldiers)
- Preventive programs must be given priority over curative care
- Health services must integrate the services of practitioners of Traditional Chinese Medicine and Western medicine
- Health care must be integrated with mass movements
From the early 1950s to 1965, before the beginning of the Great Cultural Revolution, existing facilities were renovated and new “people’s hospitals” and other preventive health facilities were built in each city and urban district. Some industrial sectors, such as mining, railways and telecommunications, and military organizations established their own hospitals, numbering around 1,500 by 1965.[18] Most of these hospitals were located in the urban areas, serving the employees and dependents of these industries. In addition, almost every government institution, enterprise and school had a health clinic which provided very basic curative and preventive services. Paramedics were trained to serve at community clinics, acting as the first-line providers of health services. Thus, the network of urban health services was greatly expanded.
Training capacity also expanded rapidly over the period. The number of graduates of medical and pharmacy schools grew from 1,314 in 1949 to 22,027 in 1965. As a result, the number of doctors of Western medicine in China increased fivefold and the number of pharmacists rose from virtually zero to 8,000 in 1965.[19] Most of the doctors and pharmacists were employed by the urban hospitals and other urban health facilities, although efforts were made by the government to deploy more health professionals in the countryside.
It should be noted that, during the 1950s and early 1960s, the development of healthcare services in urban China mainly followed the model adopted by the former Soviet Union before friendship between China and the Soviet Union ended. The majority of urban residents who were employed were covered by a traditional health care system that was implemented in the 1950s and continued right up to the mid-1990s when health reform was carried out. Specifically, this traditional health care system was administered through two insurance schemes: (1) the government-funded insurance scheme (GIS) for personnel of government agencies and institutions, including disabled veterans; and (2) the labor insurance scheme (LIS) for state-owned enterprise (SOE) staff and workers. These SOEs were enterprises of more than 100 workers each, including factories and enterprises in the railway, mining, transport, and postal industries. Insured employees virtually enjoyed free health care for work-related and non-work-related illnesses, injuries, and disabilities. They only had to pay for expensive medications. Immediate family would have half of the medical expenses for surgery and general medicines paid for by the SOE. Under a command economy with such employment-based benefits, there was significant improvement in the health of the vast majority of Chinese urban population.
In contrast, health care in the rural area was administered through the Cooperative Health Care System launched by local farmers in the mid-1950s, and subsequently affirmed by the central government.[20] Under this system, a health care fund was set up with contributions from members of a production team or commune as well as subsidies directly provided by the production team or commune. Members received medical treatment or prescriptions free or at reduced price. However, there was only limited number of healthcare providers available in the rural area, based in small clinics at the township and county levels.
This bi-furcated health care system has created regional inequality between the urban and rural populations. Whereas the urban employed could enjoy the traditional health care available in the cities, access to basic health care remained inadequate for most of the rural population in China.
The Period of the Great Cultural Revolution 1965 – 1978
In 1965 Chairman Mao made a famous speech criticizing the health sector for favoring the urban areas and calling for a radical change in priorities. At almost the same time, Mao and his political allies within the Communist Party Committee of China launched the Great Cultural Revolution, which brought political and economic turbulence to China over the following decade.
The new Ministry of Health began to make rural health development its priority policy. This resulted in the training of large numbers of “barefoot doctors” – part-farmers and part-doctors – to play a key role in the provision of rural health care, the construction of rural health facilities, and the re-organization of rural cooperatives to provide funds for rural health services.
An important goal during the Great Cultural Revolution was reduction of the inequality between urban and rural areas in the numbers of available health care workers. Many training and research centers in the urban areas were closed. High-level medical education was restructured. The five-year training program for medical and public health doctors was reduced to three years. Many doctors from urban hospitals were sent to the countryside to provide the rural residents with better health care and to supervise poorly trained rural health care workers. For example, in 1969, Gansu Province in western China sent 50% of its urban doctors to rural health facilities.[21] At the same time, new medical and public health graduates were automatically assigned to rural facilities. The number of qualified doctors in rural areas was almost doubled within ten years, while the number of nurses in rural areas increased by 137%. In addition, the construction of health care facilities in the rural areas overshadowed the urban sector. By 1975 over 85% of villages in the rural areas had a health station. By 1976, about 90% of the rural residents in the country had enrolled in the Cooperative Health Care System.[22]
In summary, the outcomes of the health sector emerging from the Great Cultural Revolution were mixed. On the one hand, the overall quality of health care in many cities deteriorated because of the collapse of the urban medical referral system involving clinics and hospitals. In addition, many health institutions, including medical or pharmacy schools, were unable to function effectively, with deleterious effects on education and research. On the other hand, the health status of the rural population in China improved dramatically, resulting from, among others, the deployment of qualified doctors, the training of “barefoot doctors,” and the further development of rural Cooperative Health Care System.
Problems of the Traditional Health Care System.[23] Under the traditional healthcare system, workers who were covered by either the government or labor insurance schemes (GIS/LIS) were provided with a relatively decent level of health care, including free diagnosis and treatment, general medicines, and surgery. In a command economy, this system guaranteed the majority of urban residents basic health care, thereby fostering social stability and economic development. However, as a result of the decollectivization of the rural economy, decentralization of decision making, introduction of management accountability, and emergence of the private sector, problems of this traditional health care system began to surface in the late 1970s.
First, there was little control over the provision and consumption of healthcare services, resulting in high medical costs, low efficiency, and tremendous waste.[24] It was estimated that about 20-30 percent of total medical costs was considered medically unnecessary. On the demand side, there was excessive use by the consumers. On the supply side, since hospitals, receiving less and less financial support from the local government, had to rely on profits from the use of high-end medical equipment and the sale of medicines to defray operating expenses,[25] many hospital-based physicians ordered unnecessary diagnostic tests or over-prescribed medicines to increase hospital incomes, thus further increasing the medical cost. Second, the broad range of medical benefits at little or no cost to workers had drained both government and enterprise treasuries.[26] Third, since health care was tied to employment and there was a discrepancy in the level of medical services received by workers employed by various enterprises, the resulting low labor mobility in turn slowed down the development of a labor market. Fourth, there was no attempt by these enterprises to pool their risks and their funds to pay for the medical expenses of their workers.[27] When enterprises experienced financial difficulties, they either contracted a low volume of health care or were in arrears with reimbursements for medical fees. Therefore, many workers did not receive the basic health care to which they were entitled. Fifth, even though private enterprises and foreign investment enterprises had developed rapidly, workers in those enterprises were not able to enjoy even basic health care.[28] In summary, the traditional healthcare system (GIS and LIS) oriented toward the urban employed resulted in high medical costs; imposed a heavy financial burden on the state treasury and enterprises; hindered labor mobility; had a low capacity to resist risk; and benefited only certain segments of society.
On the rural side, with the de-collectivization of the rural economy, and the disintegration of rural communes, the Cooperative Health Care System broke down and left the rural population stranded. This set the stage for health care reform following Deng Xiao Ping’s economic reform in 1978.
Health Care Reform (from 1980s)
Starting from the 1980s, local health authorities and enterprises began to undertake measures to reform the health care system.[29] (1) Workers were required to share with their employers part of their medical costs, normally 10 to 20 percent, with an upper limit set for out-of-pocket payment. (2) A capitation system was introduced, in which enterprises gave health care providers a fixed sum of money annually for taking care of a certain number of employees.[30] (3) In 1989, some municipalities began to set up social pooling funds to cover the medical cost of retirees, [31] while others launched pooling funds for serious illnesses. (4) In 1993, personal medical account was added to the socially pooled funds to help workers save for future medical needs.[32] However, all these reform measures were still undertaken within the framework of the traditional health care system, but did little for the masses.[33]
Emergence of Basic Health Insurance (urban). Over the years, China has adopted an incremental approach to effect reforms in various respects, such as economic reforms and labor reforms. Health care reform is no exception. In 1996, a national conference on Basic Health Insurance was sponsored by the State Council. As a result of that conference, over fifty cities became test sites of this health care reform, incorporating the above-mentioned features into the trial scheme.[34] Encouraged by the results, the State Council promulgated a landmark decree in December 1998, the “Decision concerning the Establishment of the Basic Health Insurance System for Urban Staff and Workers,” followed by the unification of the government insurance scheme (GIS) and the labor insurance scheme (LIS) in 1999 to form the “Basic Health Insurance System for Urban Staff and Workers” (in short, Basic Health Insurance). Its slogan is “low level, broad coverage.”[35] The underlying objective of this health care reform is to provide better-quality medical services at relatively cheap cost in order to satisfy the basic medical needs of the urban employed.
The general framework of this insurance is composed of a socially pooled fund and personal medical accounts, to be managed by the Social Security administration of the local government rather than by the employers. The socially pooled fund is drawn from the insurance premium paid by the employers and employees, while the personal medical accounts are designed to encourage employees to save for their future medical needs and to control waste resulting from excessive usage of medical services. Thus, the cost of medical care is to be shared between employers and employees.
Under this Basic Health Insurance, workers go to designated healthcare providers for diagnosis and treatment. Thereafter, they can fill prescriptions at the hospital’s outpatient pharmacy or at designated drug retailers. Designated health care providers are certified by the Ministry of Labor and Social Security and must sign capitation contracts with the social security administration of the local government in order to provide medical services.
This Basic Health Insurance is meant to cover all urban workers employed in enterprises, institutions, and government organs nationwide. To ensure fairness and to bring into play the initiative of workers, those who have made a significant contribution to society can have the extra benefits of a supplemental insurance from the government or state-owned enterprise. This supplemental insurance can also be offered to those who are suffering from serious illnesses. Commercial insurance is also available for those who can afford it through their employers. Unfortunately, for the unemployed, the disabled, and those who have used up all the funds from available insurance channels, medical relief is the last resort for those under the poverty line.
This health care reform consists of two other major components beside the Basic Health Insurance: the reform of medical establishments, and the reform of the medicine production and circulation system. For the purpose of this paper, I will not go into details on these two reforms, suffice it to say that
- quality and efficiency of medical personnel are to be increased, and their total number is to be decreased
- fee schedule of medical services is to be normalized
- access to health care is to be improved by actively developing community health services and incorporating these services into the coverage of the Basic Health Insurance
- medications are separately managed from medical services
- health care providers are discouraged from over-prescribing medications by setting a limit to the proportion of hospital income from filling prescriptions to the total income of each medical establishment
- centralized solicitations of bids from drug wholesalers are to be encouraged
- the franchising of retail drugstores and counters for nonprescription drugs in franchise shops and supermarkets are to be encouraged; hospital pharmacies are expected to be eventually converted into independent retail drugstores
- drug prices are to be normalized nationally, with the government setting the prices of designated medicines, listed under the formulary of Basic Health Insurance, for which patients can get re-imbursements
- the retail price of a medicine has to be printed on its packaging to prevent price gouging, while invoices based on the actual price of a medicine must be produced at every stage of sale
There are some notable changes in this healthcare reform. First, health care is now treated like an industry. The administrative-subordinate relationship between the Ministry of Health and hospitals is abolished, with the former now serving the supervisory role and the latter serving the technical-service role. Formerly, the Ministry of Health managed hospitals. From now on, the Ministry of Health only supervises medical establishments at the industry level. Second, medical establishments are now classified as for-profit and not-for-profit, with the latter receiving preferential tax treatment. For-profit medical establishments may set their own fee schedule, but must pay tax in accordance with the law. Some not-for-profit medical establishments are run by the government and receive subsidies from it. Third, there is now an extensive service system of community health centers, general hospitals, and specialized hospitals. Conversion, cooperation, merger, and grouping of hospitals are encouraged, so as to secure the rational distribution and utilization of medical resources.
As a result of this reform and the ensuing competition, the management level of hospital leadership, the doctors’ consciousness regarding medical expenses, and the quality of hospital services have improved.[36] Moreover, hospitals have either streamlined their operations or merged with others to remain competitive.
Reform in Cooperative Health Care (rural). Along with the reform of the urban health care system and the de-collectivization of the rural economy, the old Cooperative Health Care System supported by communes and production teams needed to be revised. The problem was a pressing one: China has 900 million rural people, and more than 700 million remain in the countryside and live in poor conditions.[37] In 2003, the Ministry of Health, Ministry of Finance, and Ministry of Agriculture jointly promulgated the “Circular concerning the Establishment of a New-Style Rural Cooperative Health Care System.”[38] According to this circular, the New-Style Cooperative Health Care System is to be organized, guided, and supported by the government; funded from various channels (including the central and local governments plus various cooperative entities in the countryside); and enrolled in voluntarily by individuals.
Under this pooling scheme, each farmer is to pay at least 10 Yuan a year (USD1.25) into his/her personal medical care account as an insurance premium, and the collective economic entities in villages plus the government (local and central) will inject another 40 Yuan (USD5) into this account. Then, the government will pay a maximum of 65% of his/her medical charges a year. Localities with better economic conditions may raise the amount of premium. As for workers employed by township and village enterprises, the county government will decide whether they should participate in the Basic Health Insurance or the New-Style Cooperative Health Care System (called New Cooperative from here on).
The fund from this New Cooperative is used primarily for large medical expenses and hospitalization charges. If, in a given year, an enrollee has not used any money from the fund, a regular physical checkup is allowed, to be paid out of this New Cooperative fund. It is the local county government that will determine the fee schedule and what examination items are appropriate for this regular checkup. The charges incurred on medications are determined from a list set up by the provincial government or equivalent.
Starting in 2003, each province, autonomous region, and municipality directly under the central government must select at least two to three counties (or cities) as test sites for this reform, and, after gaining the necessary experiences, gradually expand this rural healthcare reform to other counties. Any county that cannot fulfill such requirement may still coordinate its villages (or townships) in the initial stage of implementing the new system. The ultimate goal is to have the New Cooperative implemented nationwide by 2010.
Thus, in a nutshell, the Chinese system of health insurance is pluralistic and multi-layered. It is pluralistic because several sources together fund the overall health insurance scheme – government, enterprises, workers, and donations. It is multi-layered because the means of payment for medical costs consist of various levels: individual savings (personal medical account and personal funds), family assistance (supplemental), a socially pooled or cooperative fund under unified collection and management of premium (mutual aid among enterprises, institutions, and cooperative entities), enterprise insurance (supplemental), commercial insurance (supplemental), and medical relief (for people under the poverty line).
There are two major reasons for such a pluralistic and multi-layered health insurance scheme. First, since the socially pooled fund covers only the basic medical services, there is plenty of room for developing other types of insurance due to differences in income level and medical needs. Second, it is recommended that regions, industries, and enterprises that used to provide medical services above the basic level establish multi-layered health insurance, thereby guaranteeing the connection of the old and new systems as well as the steady implementation of medical reform.
By the end of 2002, about 69.26 million workers and 24.74 million retirees had subscribed to the Basic Health Insurance.[39] The increasing number of subscribers demonstrates that the implementation of the Basic Health Insurance has gained full momentum. As for the New Cooperative, it is still too early to evaluate its impact. Because of its modest funding,this New Cooperative covers only inpatient care (with a very high deductible)and leaves farmers without adequate primary care services anddrug coverage.
Current Management of Health Care Facilities
Fiscal Decentralization
For most local governments in China, the development of health care has not been a priority over the past two decades. Developing the local economy has always been given a higher priority than health care and other social services. As a result of fiscal decentralization, the proportion of income from government to hospital finance has declined significantly since the economic reform started in the 1980s. It accounted for only 8.7% on average of hospital revenues in 2000 (see Table 5 below which provides a clear picture of how sources of hospital income have changed over the past two decades).
Table 6: The composition of hospital incomes in China, 1980-2000 [40]
Items 1980 1985 1990 1995 2000
| Total income (CNY100 mill.) | 292.6 | 428.6 | 702.2 | 1,003.4 | 2,296.5 |
| % of medical service | 18.9 | 22.2 | 28.6 | 34.7 | 40.2 |
| % of drugs | 37.7 | 39.1 | 43.1 | 49.8 | 47.1 |
| % of government subsidies | 21.4 | 20.2 | 11. 6 | 7.5 | 8.7 |
| % of other source | 22.1 | 18.6 | 16.7 | 7.9 | 4.0 |
Table 7: The Chinese Government’s Share of National Health Spending,as a Percentage of Total Health Care Expenditures
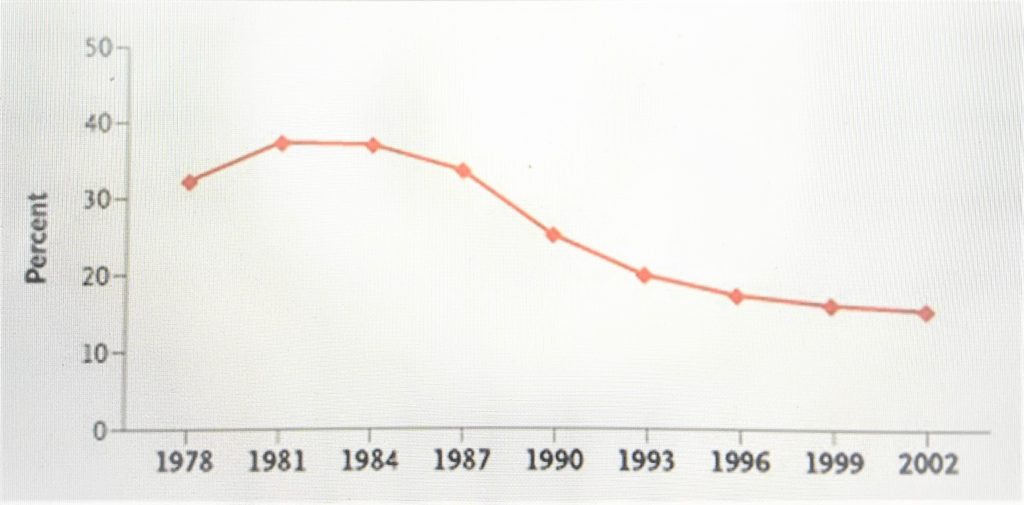
From 1978 to 1999, the central government’s share of national health care spending dropped from 32% to 15%.[41]
Financial Responsibility System
Consequently, with fiscal decentralization, hospitals and other health facilities are required to generate as much revenue as possible by charging higher medical service fees to patients in order to cover the increasing operational costs. In 2000, the percentage of hospital income due to medical services had increased significantly to 40.2%, with a significant drop in government subsidies (see Table 6).
Under the fiscal decentralization and the financial responsibility system, managers of these institutions have been given more autonomy in the management of their institutional (1) financial and (2) personnel affairs as well as (3) provision of health services.
Financially, if the health facilities have a surplus from their revenue-generation activities, the managers have the power to decide what proportion of the surplus can be used to pay bonuses and how much should be spent on investment for further development. With the support of their staff, they can set up a system that defines how bonuses should be paid to different levels or types of employee.
In personnel affairs, the health managers have a bigger say in the recruitment and firing of new staff. Increasingly, health professionals have been given job contracts instead of being offered permanent jobs as was the case previously. As a whole, human resource management in many health facilities has been improved greatly over the past two decades, but a lot remains to be done in order to improve the efficient use of health personnel.
In providing health services, health managers have often strategically developed new health services in order to generate more revenue and profits for their own facilities (e.g. through purchasing new high-tech imaging equipment). To some extent, the provision of care in many health facilities in China has been driven by profit, rather than the health service needs of the local population. The majority of district and higher-level hospitals in China have purchased CT scanners to make profits. One typical example is that the price of a CT (computerized tomogram) scan examination was once set at a level much higher than its cost.
In enhancing productivity, which has declined substantially due to increases in cost of health services and falls in utilization, managers of most hospitals have introduced an incentive system, which offers incentives for achieving revenue targets for departments, units and individual staff. The system developed in most hospitals was initially driven by a desire to increase revenue by encouraging doctors and other health professionals to increase utilization of medical services and sell more drugs to their patients. This means that the more revenue doctors generated from the provision of services or the sale of drugs, the more bonus they could get in their monthly pay. Such an incentive did increase labor productivity. However, over-prescription and overuse of high-tech diagnostic procedures and treatments have dramatically driven up the cost of medical care,[42] and made patients less trusting of their attending physicians. In recent years, these problems have been recognized and hence, some measures to improve the cost-effectiveness of services, including patient satisfaction, have been brought in to reverse the situation.
Government’s Price Reform
Before the economic reform, the prices of health services and drugs were set at a very low level by the government so that the vast majority of the population could afford them. The Chinese government started to reform the prices of health services from the early 1980s. The main purpose of the price reform was to let new higher prices reflect the real costs and enable health care providers to remain financially viable despite the limited financial support from government. Under these circumstances, a new health care pricing system was established for health services and pharmaceutical products. Provincial or municipal government agencies, led by the Price Bureau, establish higher fee schedules according to the local situation. All public health care providers and hospitals must follow the fee schedules issued by their local governments. In addition, public hospitals at and above county level are requested to self-monitor their pricing scheme.
Evaluation of Health Care Reform since 1978
This cascade of events – fiscal decentralization by the government, increasing financial responsibility of health care providers, and privatization of both enterprises and agricultural economy – can be best understood from the following three perspectives:[43] (1) the overall functioning of China’s health care delivery system; (2) disparities between China’s rural and urban areas; and (3) equity issue in accessing health care.
Overall Functioning of China’s Health Care Delivery System
In a 2001 survey of residents inthree representative Chinese provinces, half of the respondentssaid that they had forgone health care in the previous 12 monthsbecause of its cost.[44]In 2002, only 29 percent of Chinesepeople (urban and rural) have health insurance, and out-of-pocket expenses accounted for58 percent of health care spending in China as comparedwith 20 percent in 1978.[45] Yet, health care expenses are burgeoning, albeit from a lowerbase than in the United States. From 1978 to 2002, annual percapita spending on personal health services in China increasedby a factor of 40, from 11 to 442 Yuan (or from roughly USD1.35to 55). Overall, national spending on health care of all types(including public health) rose from 3.0 percent to nearly 5.5percent of the GDP. Because of the profitability of sellingpharmaceuticals and high-tech services, these items are widelyoverused. Half of Chinese health care spending is devoted todrugs (as compared with 10 percent in the United States).[46]Backed by Western capital, a new for-profit medical sector hasemerged to provide Western-style medicine in beautiful new facilitiesto China’s rich urban elite.In the meantime, the efficiency of the Chinese health care systemhas declined precipitously. With the growth of the private healthcare sector, the number of Chinese health care facilities andpersonnel has increased dramatically since 1980, but becauseof barriers to access, the use and thus productivity of thehealth care sector have declined.[47] To many in the United States,this portrait of pockets of medical affluence in the midst ofdeclining financial access and exploding costs and inefficiency may sound depressingly familiar. [48]
Disparities between China’s Rural and Urban Areas
In China’s market-based health care system, thewealth of consumers is a critical predictor of their accessto services and the quality of services, and with urban incomestriple the incomes in rural areas, urban residents have faredfar better than rural citizens. In 1999, 49% of urbanChinese had health insurance, as compared with 7% ofrural residents overall, and 3% in China’s poorest ruralWestern provinces.[49] Furthermore, the quality of care in ruralcommunities is inferior to that in urban communities for reasonsthat are familiar worldwide: the numbers and quality of healthcare facilities and personnel in rural areas are inadequate.In particular, rural communities depend on care from formerbarefoot doctors, who had little training and who now earntheir keep mostly by selling drugs and providing intravenousinfusions, a popular form of therapy for all kinds of problemsin China.[50] It has been estimated that one third of drugs dispensedin rural areas are counterfeit, enabling their vendors to earnhuge markups.[51]
Aware that their health care is poorer in quality, rural residents with serious illnesses frequently bypass local practitioners and facilities to seek care in the outpatient units of urban hospitals, leading to under-use of the former, overuse of the latter, and increased fiscal burdens on farmers who seek out more expensive, hospital-based services. Health expenses area leading cause of poverty in rural areas and a major reason that many migrate to cities seeking proximity to better health care facilities and higher wages to pay for care.[52] Regional differences in wealth also profoundly affect public health expenditures,which are more than seven times higher in Shanghai than in the poorest rural areas. [53]
These gaps in wealth, financial and physical access to care,and public health expenditures between urban and rural areasare reflected in health statistics. In 1999, infant mortalitywas 37 per 1000 live births in rural areas, as compared with11 per 1000 in urban areas. In 2002, the mortality rate amongchildren under five years of age was 39 per 1000 in rural areasand 14 per 1000 in urban locales. Urban and rural maternal mortalityrates in 2002 were 72 and 54, respectively, per 100,000. Perhapsmost shocking, in some poor rural areas, infant mortality hasincreased recently, although it has continued to fall in urbancenters, and there has been a resurgence of some infectiousdiseases, such as schistosomiasis, which was effectively controlledin the past.[54]
Gaps in health care are an important reason for growing angerin some rural districts toward the Chinese government, the ChineseCommunist Party, and China’s new, wealthy elite and they are contributingto increasingly frequent local riots and disturbances in ruralChina.[55] In a country where threats to established politicalauthority (such as the communist revolution itself) have sprungup for millennia from the grievances of an impoverished peasantry,the consequences of differentials between rural and urban healthcare carry profound political significance for the current Chineseleadership.
Equity in Accessing China’s Health Care
Equity has always been a critical issue to China’s health care system. Access to health care has primarily been based on employment – employment status, performance, and ownership of the employer – and the place of residence, i.e., the divide between rural and urban residence according to household registration. The traditional health care system, consisting of the Government Insurance Scheme (GIS) and the Labor Insurance Scheme (LIS), was designed for urban employees and was exclusive in coverage. The newly introduced Basic Health Insurance in 1998 continues this fundamental feature.
Despite these changes, the Chinese urban health care system is still characterized by the exclusion and inadequate protection of those who are uninsured and under-insured. For example, Zhuan identified five vulnerable groups in 2002 in Shanxi Province totaling two million workers or ex-workers of varying status, and a further 0.58 million of poor people, most of whom were old and chronically ill, who were covered by the government poverty relief program – with a certain guaranteed allowance for livelihood – but who had access problems to health care under the new Basic Health Insurance.[56] The five groups were: (1) employees of unprofitable enterprises; (2) unemployed workers; (3) retired workers on low pension benefits; (4) handicapped; and (5) rural-to-urban migrant workers. Apparently, all five groups were likely victims in terms of health care access because of their weak employment status in an open economy. It is worth noting that Shanxi Province had more urban poor than any other province in China at that time,[57] but the problem of health care access is not confined to Shanxi Province alone. It is a nation-wide problem. Even in Beijing, China’s capital, a similar situation has been reported. A survey conducted in 2001 by the Ministry of Civil Affairs, which is responsible for poverty relief and social welfare for the poor and vulnerable groups, revealed that three quarters of the respondents chose to treat their own illnesses without medical attention; three quarters paid out-of-pocket for their medical expenses; and only 12.2% had Basic Health Insurance.[58]
These findings should not be surprising because health care reform does not change the basis for health care system in China, which is based on employment. Even worse, economic reform has also brought about gaping differences in income. When China first reached the per capita GDP threshold of US$1,000 in 2003, many vulnerable groups were still underinsured or uninsured.[59] This is not to suggest that health care reform has not mitigated inequality in health care access at all, but there is evidence to suggest that lower socio-economic groups continue to be disadvantaged in their access to the type of health care they need when seriously ill.[60] While inroads have been made to improve equity horizontally in accessing basic health care, vertical inequity remains.
Summary
Healthcare services need to adapt to the changing patterns of need. The low birth rate has led to a fall in demand for maternal and child health services, while the aging of the population has generated unmet needs for a variety of support services. The growing number of urban poor and socially excluded people and the large rural-to-urban migration are also creating new needs. Healthcare institutions and facilities need to strengthen their capacity to monitor for, and respond to, new needs.
The Basic Health Insurance is the centerpiece of the government’s strategy for financing urban health services. The aim is to help establish this in all cities eventually. The richer cities could supplement this basic scheme. The challenge is to convince younger workers that they will ultimately benefit from it, or else they will see it as just another form of tax. This scheme currently does not cover family members of employees. This works to the detriment of middle-aged and elderly women, who are more likely to stay home rather than taking outside jobs. In addition, the present insurance scheme provides only partial benefits for out-patient treatment of chronic illness. This creates a heavy burden on some households and may in fact cost more in the long run because of the more expensive in-patient treatments.
Any health care reform is unlikely to succeed unless changes are made to the health care delivery system. The present heavy reliance on acute care hospitals for inpatient treatment and for the care of the chronic ill is very costly. More and better primary care facilities at the community level are needed. Cost-effectiveness in hospital management needs improvement, including rational use of diagnostic technologies and pharmaceutical products.
Diverse health insurance schemes are needed to improve consumer capacity to purchase needed services. Health care departments or bureaus need to strengthen their ability to monitor and regulate the performance of health care facilities. City governments will do well to actively plan for the development of their health services. The public also needs to be informed on available options in their choice of health care.
The rising number of elderly is creating a special challenge to health care. Most cities will not be able to provide them with the kind of hospital-based health care that those with full health insurance currently enjoy. Cities will be better off in meeting their needs through primary care and community support, and having them cared for in their own homes or in nursing homes. Any health insurance scheme would find it draining to fund health care for the elderly out of premiums paid by younger workers and contributions made by employers alone. Under that circumstance, governments should bear some of that cost; otherwise the whole health insurance scheme could fall flat.
For sure, it will be some time before everyone is fully insured. However, government can take other measures to protect the rest of the population. It can fund community health services and preventive programs adequately. It can encourage the development of cost-effective out-patient facilities. It can monitor and regulate the performance of the hospitals. It can reduce the over-prescription of drugs and over-utilization of health services. It can educate the public in many areas of health care. The government, under the Ministry of Civil Affairs, has begun to experiment with a safety net for health-maintenance in the poor, especially in the area of chronic illnesses, and to ensure that poor people have adequate access to essential health care.
One of the greatest challenges to city health departments is the changing nature of the populations they serve. Many localities outside city boundaries are becoming increasingly urbanized. These localities may be gradually integrated into the city. This will create many challenges to the provision of health services, the organization and financing of urban health services, and the ongoing reform in insurance schemes. As stated earlier, rural-to-urban migrants now constitute an important, but unknown, proportion of urban residents. Municipal governments need to take up the responsibility for their health care. There are two obvious reasons for it. First, these migrants are tax payers too and should be entitled to social benefits. Second, for public health reason, communicable diseases can be better controlled, as the importance of this issue was graphically illustrated during the SARS (Severe Acute Respiratory Syndrome) outbreak. The employers of these migrant workers should be encouraged to enlist them in the Basic Health Insurance. This raises difficult questions about whether insurance benefits can be portable when these migrants return to their rural homes.
For the past 20 years the government has
responded rather passively to problems encountered by the urban health care
services as the country manages a rather swift and successful transition to a
market economy. Some of these problems include rapid rise in medical cost, and
many citizens are questioning how they can cope with the heavy financial burden
of a serious illness. Furthermore, adequate and equitable access to much needed
medical care remains a problem. The government has promised to give priority to
these problems. It remains to be seen how this will all pan out.
[1] People’s Republic of China, Bureau of Statistics, China Statistical Yearbook (Beijing: China Statistics Press, 2001).
[2] China Statistical Yearbook, 2001, Tables 10.3 and 10.9.
[3] China Statistical Yearbook, 2001,Table 3.9.
[4] China Statistical Yearbook, 2001,Table 10.5.
[5] China Statistical Yearbook, 2001,Table 5.4.
[6] China Statistical Yearbook, 2001,Table 5.1.
[7] Edward Gu, “Labor Market Insecurities in China” (Geneva: International Labor Office Publ., 2003), http://www.ilo.org/public/english/protection/ses/download/docs/labour_china.pdf (accessed May 14, 2008).
[8] Sarah Cook and Susie Jolly, “Unemployment, Poverty, and Gender in Urban China: Perceptions and Experiences of Laid-off Workers in Three Chinese Cities,” IDS Research Report, No. 50 (Brighton, England: University of Sussex, Institute of Development Studies, 2001); Chun-ling Li, “The Class Structure of China’s Urban Society during the Transitional Period,” Social Sciences in China, 23, no. 1 (2002): 91-99.
[9] China Statistical Yearbook, 2001.
[10] Alan Williams, “‘Need’ – an Economic Exegesis,” in The Economics of Health, ed. Anthony J. Culyer,vol. 1 (Brookfield, VT: Edward Elgar Pub., 1991), 259.
[11] Morris Barer et al., “Aging and Health Care Utilization: New Evidence on Old Fallacies,” Social Science and Medicine 24, no. 10 (1987): 851-62.
[12] Ai-hua Ou and Yan Zhu, “Analysis of Condition of Elderly People and Their Health Service Utilization in Guiyang City,” Chinese Primary Health Care 14, no. 3 (2000): 47-8; Li-ping Zhou and Rui-zi Wang, “Analysis of Health Need and Utilization of Elderly Population in Hangzhou City” [in Chinese], Journal of Zhejiang Medical University 27, no. 2 (1998): 84-87.
[13] Yue-gen Xiong, “Social Policy for the Elderly in the Context of Ageing in China: Issues and Challenges of Social Work Education,” International Journal of Welfare for the Aged, 1 (1999): 107-22.
[14] World Bank, China National Development and Sub-National Finance: A Review of Provincial Expenditures, Report No. 22951-CHA (Washington, D.C.: World Bank, 2002).
[15] Gerald Bloom and Sheng-lan Tang, eds., Health Care Transition in Urban China (Aldershot, Hants, England; Burlington, VT: Ashgate, 2004), 14.
[16] Joshua S. Horn, Away With All Pests: An English Surgeon in People’s China: 1954-1969, chap. 8(New York: Monthly Review Press, 1971), 70.
[17] De-quan Li, “The Right Direction in Providing Health Care for the People” [in Chinese], lecture delivered at the First National Health Conference, Beijing, Aug. 7-19, 1950, reported in People’s Daily Oct. 23, 1950, Editorial,http://read.woshao.com/400327 (accessed May 25, 2009).
[18] Bloom and Tang, 18.
[19] Bloom and Tang, 18.
[20] Dong-jin Wang, ed., The Reform and Development of China’s Social Security System [in Chinese] (Beijing: Falu Press, 2001), 278-79
[21] People’s Republic of China, “History and Development of Health Care System in Gansu Province” [in Chinese], Gansu, 2000.
[22] Wang, Reform and Development of China’s Social Security System,278-79.
[23] Chack-kie Wong et al., China’s Urban Health Care Reform (Lanham, MD: Lexington Books, 2006), 14.
[24] Dong-jin Wang, “The Importance and Urgency of Sufficiently Understanding the Reform of the Health Insurance System for Urban Staff and Workers” [in Chinese], China Labor 158 (Jan. 1999): 4-7.
[25] Xiao-wu Song and Hao Liu, “The Reform of the Health Insurance System and Accompanying Measures,” in Report on the Reform and Development of China’s Social Security System [in Chinese], ed. Xiao-wu Song (Beijing: Renmin University of China Press, 2001), 83-106.
[26] Pei-yun Peng, Reform on Health Care System for Staff and Workers [in Chinese], report prepared for Social Security Department, People’s Republic of China (Beijing: Gaige, 1996), 3-21.
[27] Ibid., 4.
[28] Ibid., 3.
[29] Jia-gui Chen and Yan-zhong Wang, “The Report on China’s Urban Health Care System,” in China Social Security System Development Report 1997-2001 [in Chinese], ed. Jia-gui Chen (Beijing: Shehui Kexue Wenxian Press, 2001), 81-82.
[30] Song and Liu, “Reform of the Health Insurance System,” 89.
[31] Ibid., 90.
[32] Ibid., 91.
[33] Chen and Wang, “Report on China’s Urban Health Care System,” 82.
[34] Chen and Wang, “Report on China’s Urban Health Care System,” 83.
[35] Lan-qing Li, “The Reforms of the Basic Health Insurance System and the Health and Medicine System for Urban Staff and Workers” [in Chinese], http://www.shanghai.gov.cn/shanghai/node2314/node3124/node3125/node3127/userobject6ai269.html (accessed May 24, 2009).
[36] People’s Republic of China, “An Investigative and Analytical Report on the Reform of the Health Insurance System in Zhenjiang, Changshu, and Shanghai” [in Chinese], Social Security Research Institute, Ministry of Labor and Social Security, Nov. 11, 2001, 11.
[37] People’s Republic of China, “New Rural Medical Care System to Insure Farmers’ Health,” information pamphlet publ., March 30, 2006, http://www.china-embassy. org/eng/ xw/ t243199.htm (accessed May 14, 2008).
[38] People’s Republic of China, “The Circular Concerning the Establishment of a New-Style Rural Cooperative Health Care System” [in Chinese] promulgated by the Chinese Ministry of Health, Ministry of Finance, and Ministry of Agriculture Jan. 10, 2003.
[39] Chack-kie Wong et al., China’s Urban Health Care Reform, 123.
[40] People’s Republic of China, Ministry of Health, Annual Report, Beijing, 2001.
[41] Yuan-li Liu, “China’s Public Health Care System: Facing the Challenges,” Bulletin of the World Health Organization 82 (2004): 532-38.
[42] Therese Hesketh, and Wei-xing Zhu, “Health in China: The Healthcare Market,” British Medical Journal 314 (2004): 1616-18.
[43] David Blumenthal, and William Hsiao, “Privatization and Its Discontents – The Evolving Chinese Health Care System,” New England Journal of Medicine 353, no. 11 (2005): 1165-70.
[44] Meng-kin Lim, Hui Yang, Tuo-hong Zhang, Wen Feng, and Zi-jun Zhou, “Public Perceptions of Private Health Care in Socialist China,” Health Affairs 23 (2004): 222-34.
[45] Yuan-li Liu, Ke-qin Rao, and William C. Hsiao, “Medical Spending and Rural Impoverishment in China,” Journal of Health, Population, and Nutrition 21 (2003): 216-22.
[46] Hesketh, and Zhu, “Health in China,” 1616-18.
[47] Liu, Rao, and Hsiao, “Medical Spending and Rural Impoverishment in China,” 216-22.
[48] Blumenthal, and Hsiao, 1165-70.
[49] Yuan-li Liu, “Development of the Rural Health Insurance System in China,” Health Policy and Planning 19 (2004): 159-65.
[50] Hesketh, and Zhu, “Health in China,” 1616-18.
[51] Jim Yardley, “Rural Exodus for Work Fractures Chinese family,” New York Times, December 21, 2004, A1.
[52] Ibid.
[53] Blumenthal, and Hsiao, 1165-70.
[54] Jim Yardley, “Xin-min Village Journal: A Deadly Fever, Once Defeated, Lurks in a Chinese Lake,” New York Times, February 22, 2005, A4.
[55] Joseph Kahn, “China’s ‘Haves’ Stir the ‘Have Nots’ to Violence,” New York Times, December 31, 2004, A1.
[56] Hui-lin Zhuan, “Urban Deprived Groups in the New Era: Studying the Construction of a Health Care Protection Mechanism” [in Chinese], Market and Population Analysis, May 23, 2003, 18-19.
[57] Ibid., 20.
[58] Zhong-xiang Liu, “A Study of the Problem Related to Medical Assistance for Urban Poor,” Table 2, Sociology Department, Renmin’s University of China, 2003.
[59] Pei-lin Li, “Problems and Trends of China’s Social and Economic Developments” [in Chinese], http://chna.com.cn/chinese/zhuanti/2004shxs/483054.htm (accessed 14 May, 2008).
[60] Gordon G. Liu et al., “Equity in Health Care Access: Assessing the Urban Health Insurance Reform in China,” Social Science and Medicine 55, no. 10 (Nov. 2002): 1779-94.
CHAPTER 2: Living Through Terminal Illness in China
Living Through Terminal Illness in China
It was a cold wintry day in December 2007 when my friend Bing picked me up at the bus station in Wai-hai, China. We were going to visit the Li family in the outskirts of town.[1] There was no bus service to where we were going. Bing gave me a ride on his motorcycle. The road was unpaved. We left a trail of dust behind us as we traveled on the country road. The villages we passed had no road sign. None of the houses had any numbers on them. I would be lost in this neighborhood without Bing. Now and then, we passed a peasant on the road side, who kept a tight rein on his prized brown ox, a beast that would cost a fortune for the farmer in China. There were also peasants with poles on their shoulders, as they carried buckets of fertilizers back to their farms, or fresh produce to the farmers’ market in town. We passed fish ponds where carps, tilapias, catfishes, and perches were farmed. Outhouses were found close to the water, where human excreta would go directly into the fish ponds for natural organic recycling.
We soon arrived at our destination. In front of us were several red brick houses that remained unpainted. They looked as if they had been deserted for a while. We parked our motorcycle near by and walked along a narrow pebble-stone alley in between these houses to come to a shabbily-built shack at the back. We knocked at the door. A woman with silvery white hair answered and greeted us. That was the first time I met Mrs. Li. Her forehead was covered with wrinkles. She looked tired and exhausted, with rings under her eyes. My friend Bing had told me earlier that Mrs. Li was in her forties, but she looked considerably older than her age.
As we walked in, I could smell a heavy odor of Chinese herbal medicine. An earthen pot was boiling over in the adjacent kitchen. The living room doubled up as a bedroom. It was sparsely furnished. On the left side, close to the window, was a pallet where Mr. Li was laying. Mr. Li looked like a shell of a man, shriveled up with mostly skin and bone. His eyes were closed.
“How are you? Mr. Li?” asked Bing at Mr. Li’s crumpled form.
Mr. Li opened his eyes.
“I’m okay, considering everything,” he replied.
“How was your night?” said Bing.
“No better than any other night. I could hardly get a wink of sleep.”
“I am sorry to hear that.”
“My back has been hurting. Nothing can make me comfortable. I cannot even turn in my bed without pain,” Mr. Li said dejectedly.
“It must have been hell for you. What did the doctor say?”
“I don’t see the doctor anymore,” he said, spitting the words out with frustration.
“Why is that?”
“What’s the point? We ran out of money, and the doctor simply would not do anything for me.”
“What happened?”
“Since the removal of my colon cancer, we don’t have much money left. We sold everything we had to come up with the money for the surgery. We even had to sell our brown ox. That got us around 20,000 Yuan, but all the money just came and went when we had to pay for the medical bills. Worse still, our fate played a lousy trick on us when I hurt my back.” He sighed.
“You sound discouraged. How did you hurt your back, Mr. Li?” I joined the conversation.
“I don’t know what happened. A few weeks ago, I came down with a bad cough. Something seemed to snap in my back when I was coughing hard. I was never the same after that. I had so much pain in my back that I could not even move…” Mr. Li tried to continue, but was interrupted by some hard coughs. His face was all red and contorted with agony.
“Take it easy, Mr. Li,” I said.
“It’s alright. I want to tell you my story,” Mr. Li continued, after he took a sip of water. “My wife took me to the hospital emergency room in town. It seemed such a long ride in the mule cart. Every bump in the road would give me a sharp pain in my back.”
“That must have been rough.”
“Yeah. No kidding. It was a long wait in the emergency room. Finally, the doctor came around and examined me. Without saying much, he ordered a CT scan of my back. When I told him that I didn’t have the money to pay for it, he threw his hands up and wanted to send me home.”
“How very exasperating!”
“I…I…,” Mr. Li tried to speak, but his voice broke down with emotions. His wife took up the conversation.
“My husband was not admitted, even though I knelt before his attending doctor, and pleaded with him for compassion. You know what this doctor said? He nonchalantly replied, ‘Sorry. No money, no compassion.’ What kind of doctor is that?”
At this point, Mr. Li was able to resume speaking.
“I don’t really blame the doctor. He had to follow the hospital rules. When I needed surgery, I could not be admitted to the hospital unless I put down 10,000 Yuan as deposit. That, I am afraid, is the reality,” said Mr. Li.
“What can you do now?” I enquired.
“Not much. I cannot afford the expensive pain killers that the doctor prescribed. I can only get some relief from the herbal medicines. Maybe Tian (Heaven above) would be kind to me.”
“What do you mean?”
“I mean, taking me out of my misery.”
He started sobbing. I reached for my tissue paper and offered him one.
“I feel for you, Mr. Li. Your story touches me deeply. I hope you don’t mind me asking you a very direct question. This may sound facetious. With all this suffering, why don’t you kill yourself?”
“Thank you for understanding how I feel. I don’t mind your forthright question. I have asked myself the very same question many times during my darkest hours. Despite the pain and the dismal prognosis of my disease, I hope to stay alive for the sake of my children. I hate to see them living in this cold and merciless world without a father. I hope to be a good example to them by facing my problem head on and not running away from it. If I simply stop fighting and kill myself, what kind of example am I setting for my children?”
As I said good-bye to this family, my heart was heavy. There was a great deal of hurt, anger, disappointment, dejection, and resignation in this couple. I felt powerless to help them. At the same time, the two of them had so much love and support for one other, commitment toward their children, and a profound sense of hope that transcended the suffering. When I returned to China nine months later, I was told that “Tian had been kind” to Mr. Li.
This story demonstrates what it is like for the poor and the vulnerable to live through a terminal illness in present-day China. It illustrates most of the issues described in the previous chapter. Mr. Li was a peasant enrolled under the New Cooperative Health Care System for the rural area. This system, as discussed in Chapter One, is different from the Basic Health Insurance system for the urban population. Because of its modest funding, this New Cooperative covers only inpatient care (with a very high deductible), and requires a significant deposit on admission to hospital, thus leaving many peasants stranded without adequate health care services and drug coverage. This heart-rending story is but one of many that I heard in my field work in China.
We will now examine some Chinese perspectives on suffering, on life’s meaning, and on “good” death.
Chinese Perspectives on Suffering
Chinese people often look to their traditional beliefs for enlightenment and wisdom to transcend their suffering. These beliefs include Buddhism, Confucianism, and Taoism. Even though Confucianism has generally the greatest influence on the Chinese way of thinking, Buddhism has the most to say about suffering. The Buddha taught four Noble Truths about life:[2] (1) that there is suffering in birth, aging, illness, death, and loss when we cling too tightly to these five aggregates; (2) that this suffering originates from our cravings (for sensual pleasures, existence, etc.); (3) that there is an end to this suffering if we can relinquish our cravings; and (4) that there is a path of practice that can end our suffering by letting go of our attachment to the body, feelings, perceptions, thoughts, and consciousness.[3] This path of practice is eight-fold, consisting of steps that abandon hindrances to awareness: having the right mindfulness, right view, right concentration, and right intention/resolve; as well as steps that develop qualities to expand the clarity and range of one’s awareness: exercising the right speech, right action, right effort, and right living. Geoffrey DeGraff points out that these steps remind us of the Serenity Prayer in Christianity (traditionally attributed to Richard Niebuhr): the first four representing the mind’s acceptance of things that cannot be changed, and the latter four representing one’s actions to change things that can be changed.[4]
In contrast, Confucius believed that suffering comes from Tian (“Heaven above”). Heaven above is regarded as the governing authority of the whole universe and the final judge of right and wrong. The emperor was regarded as the Son of Heaven, who had the mandate from Heaven to rule the country. If he was not moral, Heaven would cause the world to suffer. When the emperor did not see to it that there was water for irrigation, that canal barges could transport rice to the famine areas, that floods were prevented, and that roads were safe for traveling, the people would suffer. The people then could have the right to determine whether or not the ruler still had the mandate. They could rebel. When the rebellion became successful, a new mandate from Heaven would be given to the new leader and the next emperor of a new dynasty. This has been the story of China, dynasty after dynasty, for many years. However, even though it is believed that suffering comes from Heaven, the people can still do something about it to alleviate their suffering, either by changing the government or by working harder to overcome their adversities, such as increasing production or setting up cooperatives to serve each other’s needs. The belief in a relationship between Tian and labor is illustrated in my interview with Mr. Li, whose story opens this chapter. Mr. Li, as a farmer, believed in a Tian (Heaven above) that would shower blessings upon him and bring fruit to his labor, as well as relieving his unbearable pain and suffering.
Like Buddhism, Taoists see suffering as being inevitable in life, in the nature of being born, aging, body deterioration, death, and losses/separation. Previous actions may also impact our present in negative ways (karma). They are all part of the natural way (the Tao), and as such, they should be accepted with equanimity. To the Taoists, attachment and ego are the two main causes of suffering. We suffer from loss when things, persons, or relationships, which are by their nature impermanent, slip through our grasps. Most forms of suffering arise because we do not realize our true self. Suffering comes from the inventions of our own mind, and from our inability to deal with our egoistic thoughts (when our thinking becomes futile), our emotions (like fear and hatred), our perceptions (like false hope), and our desires (like covetedness). Sometimes suffering may be even caused by our compassion, for the Taoist argues: “How can anyone filled with compassion be totally happy as long as there is still suffering all around?” Taoism advocates the ideal of returning to the simple and natural way of life (the Tao) as a way of coping with suffering and with the vicissitudes of life.
Even though the word “suffering” never appears once in the Tao Te Ching, the basic text of Taoism, this classic text deals extensively with suffering by focusing more on the solutions to the problems. It does so in a light-hearted way with insightful metaphors, as if taking suffering too seriously would only trap one deeper into suffering. If attachment and ego cause suffering, then the answer to cope with suffering would be in the way of detachment and acceptance. [5] It has to start from our self, our ego. The Tao Te Ching tells us to:
Free yourself from desire; you realize the mystery. Caught in desire, you see only the manifestations (of suffering).[6]
Empty your mind of all thoughts. Let your heart be at peace. Watch the turmoil of beings, but contemplate their return. Each separate being in the universe returns to the common source. Returning to the source is serenity. If you don’t realize the source, you stumble in confusion and sorrow. When you realize where you come from, you naturally become tolerant, disinterested, amused, kind-hearted as a grandmother, and dignified as a king.[7]
Express yourself…If you open yourself to loss, you are at one with loss and you can accept it completely. Open yourself to the Tao, then trust your natural responses; and everything will fall into place.[8]
Thomas Leung, a noted Chinese-Canadian philosopher who had explored the teachings of Buddhism, Confucianism, and Taoism in depth before he became a Christian, suggests that suffering is not a “being” that comes to us because of karma. We suffer not because of our sins or our misdeeds in previous lives.[9] Like the Taoist, he sees suffering as a perception of our mind when experiencing losses. It can be loss of comfort (feeling pain as in birth from the womb); loss of youth (aging); loss of health (illness); loss of life (death), and loss of all that is valuable to us (bereavement). This suffering can result from afflictions that affect us and affect others, as well as from natural disasters.
As a Christian, Thomas Leung proposes that suffering can be redemptive with a positive meaning. When Jesus suffered and died, he was doing it for all humanity. Jesus did not harbor any bitterness, indignation, wrath or retaliation; instead, Jesus’ heart was full of sorrow, compassion, endless love and forgiveness for all who had rejected him. In his heart, he only has our best interests in mind. He died for us so that we can live. Through his suffering, Jesus exemplifies how much he shares our suffering and how we can learn from him in sharing others’ pain. The Apostle Paul also reminds us how we can comfort others just as we have been comforted in our tribulations.[10]
Thomas Leung has suggested a number of steps for us to overcome suffering. These steps are in fact a blending of Chinese cultural beliefs and Christianity.[11] First, we can try to avoid asking why we suffer, but strive to change our attitude toward suffering, perceiving it in a more positive light and believing that, like all things, it will come to pass. Taking actions to avert suffering does not always work. Perhaps it is better to accept that suffering is part of life. It is as natural as breathing in and out. Acceptance itself is an action through inaction. Taking no action is, in itself, an action (wu wei). Suffering befalls every one. Do not take it personally. We should learn to live with it rather than letting it drag us down. Instead of bemoaning what we do not have, we can simply give thanks for what we do have. We will be a lot more content that way. Finally, Thomas Leung suggests that we learn to love and forgive. We will feel better in our own suffering.
Chinese Cultural Beliefs
The history of China and her people abounds with suffering. Earthquakes, floods, droughts, and hurricanes often claim thousands of lives. So do wars and famines. Thus, Chinese people generally begin with the assumption that life is mostly negative and beyond human control, and in their coping with suffering, they often turn to their cultural beliefs and their value system, which consists of strengths and virtues that have enabled them to survive extreme adversities. Let us now examine the following cultural beliefs which are often considered widespread and dominant in the Chinese culture. [12]
Uncontrollability of the World
Heaven determines what happens on Earth. Chinese people perceive the external world as largely beyond their control. Individuals are not able to prevent or control powerful forces of nature and political forces that impact their lives. Historically, Chinese people rarely had the power to select their government through voting. Dynasty rule was mandated by Heaven, but in the process of government changes, tens of thousands of lives may be sacrificed. For the peasants, their livelihood was at the mercy of the elements as well as robbers and corrupt government officials. War after war ripped the country apart. Is it little wonder that the Chinese people have found it necessary to accept the harsh reality and shape their thoughts and behavior to allow some sort of sanity and contentment? Thereby Confucianism, Buddhism and Taoism bloomed in China.
Ubiquity of Change
To the Chinese people, the world is not only uncontrollable but also unpredictable. Without the ability to control the world, the ordinary person has found it impossible to predict how things will turn out in life. Who would have thought that overnight dynasty could change hands, and the workers would become the elite? Who would have thought that overnight, university professors and scholars would be sent to the country side and become peasants? Who would have thought that overnight, children would be turned against their parents, and parents against their own children? But such was the harsh reality. Life was as unpredictable as the weather. Confucius tried to infuse order and stability into chaos, whereas Taoism emphasizes the need to be flexible like water. Taoism, in fact, teaches that virtues like filial piety and patriotism are nothing but our desperate efforts to cope with the changes in our broken families and fractured country.
“When the great Tao is forgotten, goodness and piety appear.
When the body’s intelligence [13] declines, cleverness and knowledge step forth.
When there is no peace in the family, filial piety begins.
When the country falls into chaos, patriotism is born.”[14]
Buddhism teaches impermanence of worldly things and that life as we know it is just a delusion. All these teachings have prepared the Chinese people to face the vicissitudes of life with equanimity.
Fatalism
As a result of the first two beliefs – uncontrollability and unpredictability of life – Chinese people have generally accepted fate or destiny as being determined by some cosmic forces beyond their control. [15] “Fate has dealt me a rotten card when my son was born with this congenital heart disease,” one mother said to me. She had given up in trying to figuring it out. Fatalism recognizes the limits of rationalism and opens the door to a transcendental reality that is shrouded in mystery. To many, only sages have the great spiritual insight into such a transcendental reality. Fortune tellers abound in China, allegedly offering the superstitious a glimpse into the future through divining and palm reading. Feng shui is also widely practiced in modern China. All these are simply attempts to retain some sense of control over one’s self and one’s external world. This belief in fatalism makes unexplainable adversities more bearable. When this mother whose son was born with this heart condition attributed her misfortune and suffering to karma, fate or bad luck beyond her control, she was considerably relieved of shame and guilt.
Duality of Nature (the Yin and the Yang)
Emphasized by Taoism, this belief in duality recognizes the co-existence of opposites and accommodates discordant ideas. The symbols of Yin and Yang express best the dynamic balance between opposites in human nature as well as the human condition. From the Chinese perspective, there is generally no clear distinction between curative and preventive medicine, since the same principle – the restoration of balance within the biological systems – applies. Similarly, Chinese in general do not claim that a positive outlook can get rid of suffering or claim that virtues can prevent evil from occurring. Chinese people have learned from past history that evil and suffering will remain with us no matter how hard we try to avoid or prevent it. The key is accepting the inevitable and integrating the opposites: the positive and negative aspects of suffering, as well as the good and the bad. By embracing both the bright and the dark sides, there would often be personal growth. Wong thinks that this dualistic approach is superior, because “any individual is only as strong as his or her weakest point. Eventually one will pay a high price for turning a blind eye ton one’s Achilles’ heel.” [16]
Collectivism
Collectivism is a term used to describe any moral, political, or social outlook that stresses human interdependence and the importance of a collective instead of separate individuals. Collectivists focus on community and society, and seek to give priority to group goals over individual goals.[17] Confucius’ teaching places a heavy emphasis on collectivism with respect to state and society. As a result, collectivism is widespread in East Asian cultures.[18] Good working relationships (guanxi) are critical in these cultures, and so is loyalty to family, friends, and country. Collectivism contributes to the social capital, and increases the likelihood of collective power to defeat a common enemy. When a terminal illness hits one member of the family, the other members of the family or related communities (of neighbors or fellow believers) would rise to the occasion to offer help.
Utility of Efforts
This belief reminds people of their personal responsibility to do their very best in areas where they can exercise some control or demonstrate some ability to shape the future. These areas include work ethics (being studious and conscientious), self-cultivation efforts (in acquiring various virtues), and relational efforts (filial piety, loyalty towards friends, respect for authority, and harmony within the family or group). The story of “The old fool who tries to move mountain” teaches us that the utility of efforts extends across generations and incorporate the masses. According to the story, onlookers were puzzled by an old man who was digging at a mountain side with a shovel. “I am trying to remove this mountain so that we don’t have to climb over it to get to the next village.” “But, sir, you are old, and this is a monumental task,” they said. Wiping the sweat from his forehead, the old man answered, “Yes, I am old, but my children and my children’s children will continue until this job is done. Other villagers may also join in, you know.”
Strengths and Virtues in Coping [19]
Such cultural beliefs have played a significant role in the development of certain strengths and virtues that are valued by the Chinese people. The belief in uncontrollability of the world brings out strengths like acceptance, endurance, and self-transformation. If the outside world cannot be changed, then at least we can change ourselves, such as our desires, our perceptions and our attitudes. Acceptance here means more than cognitive consent. It involves surrender of one’s ego and acceptance of one’s fate. Endurance means more than goal-persistence. It involves wise retreat and subsequent return (just as Mao Ze-dong conducted his guerilla warfare). A popular Chinese idiom says, “As long as the green mountain remains, there will always be a supply of firewood.” The idea is that as long as we stay alive and endure whatever we have to endure, we can always stage a comeback in the future. Similarly, self-transformation means more than cognitive reframing. It involves spiritual transformation and enlightenment as well.
The belief in ubiquity of changes leads to strengths in hope, flexibility, and resourcefulness. It is precisely in the face of adversities and at the brink of despair (hopelessness) that hope is likely to arise. In Mr. Li’s situation, who would have expected that coughing could bring on such unbearable pain in the back? Who would have foreseen Mr. and Mrs. Li drained of their life savings? Who would have imagined that a doctor would say something like that? When circumstances could not be changed, Mr. Li turned to a will for meaning. He found it. That meaning gave him hope.
The belief in fatalism favors strengths in acceptance, faith and transcendence. It recognizes that rationality has its limitations. Mr. Li talked about a Tian (Heaven above) that exerts great power over life. His plea for mercy from above demonstrated a faith in providence from a higher power. This same faith has been held by the Chinese people for centuries. Many even try to decipher the will of Heaven, or seek counsel from feng shui practitioners, since they believe that fortunes are determined by the will from above.
The belief in duality leads to strengths in open-mindedness, tolerance and accommodation. This belief favors the middle-path integration and holistic thinking, rather than the either-or kind of linear dichotomous thinking. Mr. Li was able to understand the dilemma that the hospital doctor faced. Even if the doctor were compassionate, his hands would be tied by the hospital regulations. Mr. Li appeared to have accepted that reality. By embracing all of life, both negative and positive, one could better tolerate suffering. Balance is the key to contentment and bliss. Chinese often say that strength may be hidden in one’s meekness, or virtue may contain the seed of its own destruction. Thus, it is generally considered unwise to disparage meekness or to gloat over one’s forte. When Mrs. Li knelt down before the doctor, pleading for compassion and mercy, there was such fortitude hidden in that meekness. Her love for her husband would not make her stop at humbling herself if that could bring her husband a measure of comfort.
The belief in collectivism leads to strengths in cooperation, altruism, and social capital. It also results in more stable families and organizations. There is strength in numbers when the problem is too big for any one individual. Mr. Li had the support from his wife and his children. This helped him to cope with his suffering.
The belief in utility of efforts leads to strengths in conscientiousness, hard work and responsibility. If fatalism encourages dependence on providence, then utility of efforts favors independence of individual efforts. Let me now turn to another story that may help to demonstrate this point.
I met Ms. Zeng in Xin-hui, Guangdong, China more than a year ago in December 2007. [20] A common friend introduced us. I was told that Ms. Zeng was being treated for lymphoma at the time. On that bright sunny day, my friend and I arrived at Ms. Zeng’s place of work, a meticulously clean beauty salon located in a cul-de-sac. It was Saturday morning around eleven, usually a busy time for customers to come and get their hair done for the weekend festivities. We were surprised however to see the salon empty except for Ms. Zeng, watching TV by herself. Her hair was sparse. Her cheek was sunken. Her complexion was dark around the face. Her brow was furrowed. She looked older than the 33-year-old I expected to see.
“How are you doing?” I greeted her as we stepped in.
“I don’t feel so good. This chemotherapy has really knocked me out. I can’t eat. I can’t sleep. I feel tired all the time. This has affected my work and my family. Look, even my regular customers are staying away. They avoid me like the plague.”
“I am sorry to hear that.”
“First the doctor said I needed surgery. After the surgery, just when I thought I could move forward, I was taken aback by the news that my disease had spread. This chemotherapy is very expensive. We don’t have much money left.”
“You sound disappointed and worried. All this treatment must have been hell for you.”
“Yeah. Sometimes I wonder what I have done to deserve such a turn in my fortune.”
“Hmm. It’s hard to figure it out.”
“You know, we may even have to sell this salon. I am sad to see it go. I have worked so hard to build up the business.”
“What are some of the other alternatives?”
“My husband has suggested that perhaps we can open up the salon to other hair stylists on an assignment basis. They use our facility, and they pay us a percentage of what they make. What do you think?”
“That sounds like a workable plan. When there is a will, there is a way. How’s your husband?”
“He’s been very supportive, but I got upset at him for no good reason the other day. I did apologize to him.”
“Any children?”
“Yes. I have three daughters. They help me to clean things up in the salon whenever they can. I feel so blessed having them.”
“Good to hear that your family is very supportive. With all these upheavals in your life, how do you feel about your life right now?”
“Well, to be frank, I don’t know how I got into this jam. I try to be a good wife and a good mother. I worked very hard to save up enough to start this business. I don’t smoke either. Why this cancer? Life is full of hard knocks, isn’t it? But I am not going to take it lying down. I have been a fighter all my life. I am still young, and I believe that I still have a lot of living to do. Wouldn’t you say so?”
“That’s good to hear. What kind of a life do you like to live?”
“I enjoy freedom most of all, freedom to choose what I want. A high quality of life is very important to me. I am not saying I like to throw money away. I am referring more to decision-making about my own health, the choice between life and death.”
“What do you mean?”
“I am referring to things like the Advanced Directive and the Physician Assisted Suicide. When my quality of life has deteriorated to a point where I feel life is no longer worth living, I hope to be able to direct my medical care along lines that I prefer, rather than being a burden to others.”
“I see what you mean.”
“But until then, I hope to live life to the fullest. Life is filled with such wonderment and awe. I hope to spend more time with my husband and with my children, holding each other in sweet embrace. I hope to work creatively as a hair stylist as long as I am able to. I hope to continue gardening and watch in awe the flowers bloom after I plant the seeds. They say cats have nine lives. I only have one. Might as well enjoy the time I have now.”
There are a good number of people in China, especially the younger ones, who feel the same way as Ms. Zeng. They believe in karma, the universal principle of cause and effect, which proposes that the effects of all deeds are viewed as actively shaping past, present, and future experiences. In other words, suffering or misfortune may be the result of some past misdeeds. Whatever the cause of her suffering, Ms. Zeng did not brood over it. Instead, she had chosen to shape her own future. She was eager to exercise at least some degree of control over her own life, even if death is knocking on her door. She accepted the rotten card that life had dealt her, but she continued to pursue her meaning and purpose in life, with the hope of living life to the fullest. Who can argue with that? Despite the obstacles she and her husband had to face, the belief in the utility of efforts has served them well in coping with her illness and its consequences. They learned to accept both the good and the bad, and be open-minded and resourceful. With these strengths, they were able to take things in their stride, and find a creative way (such as the sharing of facility) to solve their problem.
Chinese Perspectives on Life and Meaning of Life
The following image demonstrates how three Chinese sages perceive life differently.

The Vinegar Tasters, an old Chinese painting (copyright has expired)
The Vinegar Tasters is an allegorical image representing the philosophies of Buddhism, Confucianism, and Taoism (Daoism) toward life. [21] It depicts three men dipping their fingers in a vat of vinegar and tasting it; one man reacts with a bitter expression, one reacts with a sour expression, and one reacts with a sweet expression. The three men are depictions of Buddha, Confucius, and Lao-zi. They represent the three major philosophical traditions of China: Buddhism, Confucianism, and Taoism. Each man’s expression represents the predominant attitude of that tradition toward life. A Buddhist sees life as bitter, dominated by pain and suffering. A Confucian sees life as sour, because society is in chaos, with the present out of step with the past. And, a Taoist sees life as sweet and fundamentally good in its natural state.
Some people have described this depiction as the “Comedy of Life.” Some have interpreted this painting in a more conciliatory way. Since the three men are gathered around one single vat of vinegar, it can be interpreted that all three teachings are actually one. This may have some truth in it, because after all, these three traditions have been known to influence each other in the long history of China. For instance, Taoist teaching was infused into classical Confucianism to give rise to Neo-Confucianism. In present-day China, it is not uncommon to find someone subscribing to beliefs from all three traditions.
Buddhists generally believe that life is suffering caused by attachment to our desires. Thus, the meaning of life is (1) to end suffering through detaching oneself from cravings and various attachments that are physical, psychological, social and spiritual; and (2) to attain as a result a state of eternal bliss (nirvana) or awakening, which can mean freedom from worries, fabrications, and troubling thoughts, as well as the end of repeated cycles of birth, aging, sickness, and death. [22]
Confucians emphasize normalliving as the meaning of life, saying that we can seek “the ultimate meaning of life in ordinary human existence.” [23] They recognize values or virtues in discipline and education. They believe that the good in life can be achieved through human reason and strong relationships with others (guangxi) to maintain order and harmony.
Taoists, on the other hand, believe that “bitterness and sourness come from the interfering and unappreciative mind. Life itself, when understood and utilized for what it is, is sweet” [24] and fundamentally good in its natural state of Tao. Since all things are originally from Tao, humankind would have to return to the source of, or reunite with, Tao by way of self-cultivation and self-realization. For the Taoists, the meaning in life is to realize the temporal nature of this worldly existence and look forward to reunion with the Tao some day. “Only introspection can help us find our innermost reasons for living…the simple answer is here within ourselves.” [25]
It should be kept in mind that meaning in life is not the same as reason for living. This term, reason for living, generally points to a personal meaning of life that has ultimate existential significance. Based on our value system, there may indeed be many significant meanings in our lives. However, the one that stands out as my “highest value” and supersedes the others in significance is likely to be my reason for living. Mr.Li hoped to stay alive for the sake of his children.[26] They were his reason for living. For Ms. Zeng,[27] quality of life[28] was her reason for living. In my field work, the terminally ill often wondered if they had any reason for living when they found their values and quality of life drastically diminished. Indeed, the question “Why do I live?” has been asked many times by those who continue to live against tremendous odds, or face a life full of pain and suffering. These people often wonder if there is a meaning in their lives that makes life worth living. This meaning is concerned with the significance and possible purpose that may be attributed to human existence. [29] It is strongly linked with one’s positive values in life, since the purpose of one’s life generally is to increase whatever is of intrinsic value.
Human being appears to require meaning. It is part of our human nature. Our perception is organized in such a way that we instantaneously pattern random stimuli. For example, when confronted with a broken circle, we automatically perceive it as complete. We organize external stimuli automatically into figure and ground. Some people will focus on the figure, whereas others may instead concentrate on the ground. This may explain why there are differences in cultural beliefs, values, and practices. Similarly, when facing existential reality such as meaninglessness or death, individuals tend to search for a pattern, an explanation as to why, or simply a meaning of life, a reason for living. Invariably, when the existential reality defies patterning, we feel uneasy until we can fit the situation into a recognizable pattern. Many people find it difficult to accept a terminal illness, especially in the younger age group, or in situations that defy any rhyme or reason. In my field work, one daughter could not understand why her mother had end-stage lung cancer even though her mother had no smoking history or family history of lung cancer. [30]
Another reason why we need meaning is that, not only does it tell us why we live, it also tells us how we should live. This relates to our purpose in life which, in its most general sense, is the anticipated goal which guides human actions in living. Hope, as the anticipation of achieving a realizable good, is related closely to this purpose of life. Hope provides meaning that sustains us. It explains why life, despite its bitterness and torments, can still be meaningful, and it guides us in living. This author takes the position that every living human person has a purpose in life, even though this person may not be aware of it.
Chinese Perspectives on “Good Death”
What is “good death?” This phrase is called an le si in Chinese and Japanese. It simply means “dying in peace and free from suffering.” In a contemporary sense, it is often understood as either passive euthanasia (such as withdrawal of life support in the critically ill) or active euthanasia (such as Physician Assisted Suicide, or “mercy killing” as generally known in China for the terminally ill). Peace at the time of death is the fervent wish of every Chinese.
What is “good death” in traditional Chinese philosophies? Confucians generally believe that it is dying for a worthy cause, and that virtue is bigger than life itself. One should be “willing to die to preserve virtue.” [31] As discussed earlier, Buddhists believe that death is the way to achieve enlightenment through the cycle of re-incarnations or rebirths. Taoists believe that “good death” is natural death.A person returns to nature (or Tao) upon death. Death and life are one, merging with one another. “Death, like life, is an illusion: there is no beginning and no end. There is only the endless flow of Tao. The man of Tao has no fear, for he walks with Tao.” [32] Tao Te Ching tells us, “If you realize that all things change, there is nothing you can hold on to. If you aren’t afraid of dying, there is nothing you can’t achieve.” [33]
Western moral values that are in favor of Physician Assisted Suicide (PAS) have struck a resonant chord in Confucian ethics as well. First, a strong case can be made for PAS when it is based on benevolence(ren 仁), which is a fundamental virtue in Confucianism. [34] Ren is benevolence, based on compassion and respect, manifested toward one’s parent or fellow human beings. Seeing others suffer would often cause intense pain in those who are compassionate. Chinese tradition has long associated this virtue ren with physicians, who are supposed to have a compassionate heart and a compassionate art of healing (ren xin, ren shu). This benevolence based on compassion would be in support of PAS.
Second, in Confucianism, “quality of life” in the moral sense has long been valued higher than life itself. While accepting that life can be “living hell” for many terminally ill, Confucian ethics can allow these people to be liberated from a life of bondage, when their quality of life is at its lowest ebb. Confucians do not subscribe to “sanctity of life,” but would consider PAS justified for the sake of a higher quality of life. [35]
Third, there is the issue of dignity. Some terminally ill patients consider it a humiliation and a loss of dignity when they lose control of their bodily functions. To them such an assault can be more intolerable than physical pain. Historically Confucianism has endorsed suicide with dignity in order to avoid humiliation, disgrace, and dishonor when hostile forces (from enemies, imperial authority, or oppressive government) threaten. In these cases, suicide would be the last resort, especially when there is no available love and support from family and friends. In the contemporary case of PAS, Ping-cheung Lo points out the fact that the assault on human dignity comes from an internal source (disease, old age, bodily and mental deterioration) and is therefore a universal human phenomenon. Unless sickness, aging and death are considered as enemies, it is difficult to see how Confucian ethics would find the deterioration of our bodily functions an assault on human dignity. [36]
Fourth, there is the issue of self-determination. In Confucian ethics, individual autonomy has not been a widely cherished value; [37] nor has it been discussed much in the context of human rights. The extent of personal freedom is often determined in the context of family and communal considerations.
In a nutshell, Confucian ethics is concerned mostly with the moral nature of suicide, asking if it is morally justifiable to permit PAS in some cases, based on compassion and “quality of life” issues, rather than endorsing all suicides based on the dignity issue and individual autonomy. After all, the Confucian scope of filial duties includes taking care of our own body which is a precious gift from our parents. Ceng-zi, one of Confucius’ students, is portrayed in the Analects as gravely ill and near death. [38] He bids his students to look at his hands and feet, and quotes lines from the Classic of Poetry: “All my life I have been taking care of this body as part of my duty to my parents. It is only now (near death) that I can be sure of being spared from fulfilling this duty to my parents.” [39] This very idea, that one must keep one’s body intact as a duty of gratitude to one’s parents, has remained a central idea in Chinese culture. [40]
In a cross-cultural comparison, Ping-cheung Lo points out that autonomy, which is highly valued in Western culture, is not so valued in the Confucian mind.[41] Thus, it should not come as a surprise to find only limited endorsement of PAS by the Confucian tradition. Moral differences can occur because of the differing emphases given to values that are shared across cultural traditions. Thomas Kasulis offers a visual metaphor: what is foreground in one culture may be background in another culture.[42]
Similarly, Buddhists are not unanimous in their views on PAS either. Buddha’s teachings do not explicitly deal with it. There are three instances of suicide in the Pali Canon:[43] those of the monks Channa, Godhika, and Vakkali. All three monks are seriously and painfully ill and appear to have ultimately taken their own lives. It seems that none of them were enlightened arahants [44] before their death, although they may have attained enlightenment at the moment of their death.[45] Apparently, the enlightened status of these monks is an important factor for Buddhists in condoning their actions, because an enlightened person is not destined for further rebirth. Enlightenment, as defined here, refers to a person’s state of mind – peaceful, free of anger, hate or fear.
Buddhists regard death as a transition. The deceased person will be reborn to a new life, whose quality will be the result of their karma. This produces two problems. We don’t know what the next life is going to be like. If the next life is going to be even worse than the life that the sick person is presently enduring, it would clearly be wrong on a utilitarian basis to permit PAS, as that will shorten the present bad state of affairs in favor of an even worse one. On the other hand, PAS is permitted for those who are enlightened, because they would not have to go through any more rebirths. The second problem is that shortening life interferes with the working out of karma, and alters the karmic balance resulting from the shortened life. Buddhists work with the premise that when the person who is suffering considers suicide, this person has allowed the physical suffering to cause mental suffering, putting the mind in a bad state, and leading to an error in judgment.[46]
Furthermore, taking away life, whether it is one’s own life or another, is untenable. In Buddhism, the very first precept for good living is the abstinence from destroying life. This applies to life of all grades, both human and animal. And the precept is equally binding on both clerics and lay persons.[47]
The Japanese Buddhist tradition has included many stories of suicide by monks, and suicide was used as a political weapon by Buddhist monks during the Vietnam War. But these were monks, and that makes a difference. In Buddhism, the way life ends has a profound impact on the way the new life will begin. So a person’s state of mind at the time of death is very important – they should be peaceful, free of anger, hate or fear.
Suicide was also a significant part of the Japanese samurai tradition. The samurai ritual of seppuku came very close to euthanasia indeed – an assistant would behead the one doing the seppuku in order to hasten death. The samurai’s motivation for suicide was similar to that of the person seeking PAS: either they had lost a battle and would be killed by their enemies (the analogy is that the terminally ill had lost their battle against the disease which would then become fatal) or they had been so badly wounded that they could no longer be useful members of society (in a similar analogy, the critically ill patients are no different). In line with Buddhist thinking, the seppuku ritual laid great emphasis on the state of mind in the suicidal person during the action. In summary, these cases suggest that suicide (including PAS) is only permissible for people who have achieved enlightenment and that the rest of the people who have not should avoid it.
In Taoism, the “good death” is the natural death. All things (including human beings) have their origin in the Tao, and we return to the source of life (the Tao) when we die. This understanding of oneness with the Tao leads us to an appreciation of life’s events and our place within them as simple miraculous moments which “simply are” in the present. Just like day and night, the Yin andthe Yang – the dual nature of all manifestations of the Tao – life and death are the two equal and complementary parts of nature. Where there is life, there is death. It is inevitable. All living things die, and from death life springs forth. Nature, like the four seasons, manifests itself in a harmonious cycle of constant changes. Thus, death is only natural and should not cause undue anguish.
Taoism also sees existence as interplay between three elements: (1) the individual; (2) society and its artificial values; and (3) the principles of nature or Tao. In order to lead a contented life, one must understand one’s own internal wants and needs, the values of the social structure in which one lives, and the principles of nature. The interpretation of the meaning of life and death also depends not only on what one desires and needs, but also on one’s own culture and social construction as well as the principles of nature.
Much of the essence of Tao lies in the art of wu wei (action through inaction) which means that taking no action is, in itself, an action. However, this does not mean “sit doing nothing and wait for everything to fall into your lap.” It describes a practice of accomplishing things through proper action by knowing when to and when not to act according to one’s personal capabilities and desires, as well as knowing one’s place in nature (Tao). In other words, by trusting one’s nature rather than mental contrivances, one can find contentment without a life of constant striving against forces real and imagined. Thus, a Taoist strives not to intervene in the paths of others.
Taoists see justification, based on compassion (one of the three cardinal virtues in Taoism [48]), in allowing the terminally ill to die naturally by forgoing aggressive medical procedures. However, Taoist ethics would have difficulty with any type of PAS. To take an active measure to intentionally kill someone is to act against the Tao. It is intervening with nature in the worst sense. In contrast, a natural death is a “good death,” imbibed with peace and dignity.
When pain is intractable, and suffering seems interminable, PAS (“mercy killing”) seems to be a personal preference by many Chinese, as shown in multiple surveys involving various population samples.[49] However, it should be kept in mind that the sample sizes were relatively small (maximum 171) and most of the people surveyed were city dwellers, which may have introduced a sampling bias into such data collection. After all, close to 60% of the Chinese population are peasants living in the country.
When it comes to accepting PAS for one’s parent, the opinions in the surveys are not as clear. This is not surprising, because filial piety plays an important role in traditional Chinese society. Children are expected to do their best to care for their sick parent. In the case of a parent suffering from a terminal illness, children may feel that they are abandoning their parent by following his/her wish to have life terminated. On more than several occasions, I have seen them torn in such a request. They felt completely powerless when they saw their parent suffer. They felt even worse when their parent expressed the wish to die so as to relieve their financial burden. I sense real guilt in the children.
Despite many requests for “mercy killing,” [50] China has so far not legislated PAS as yet. No institution or person is permitted by law to engage in this act. Hospitals have so far rejected such requests, but have sometimes allowed passive euthanasia (the withdrawal of life support systems) in accord to the demands of patients or their families. In practice, PAS is often done in secret, or through the “double effect” of injecting large doses of narcotic analgesic for the “primary” purpose of “pain relief.” [51]
So far, in this chapter, I have provided a
brief glimpse of what it was like to live through a terminal illness in China,
and how the Chinese people perceived and coped with such suffering. We have also
looked into the meaning of life and the concept of suicide as perceived by the
Chinese people. In the following chapters, I will attempt to incorporate into
our discussion the Western philosophical perspectives on meaning of life and
hope as they pertain to suffering in the terminally ill.
[1] Interview #6, Appendix.
[2] Donald S. Lopez, Jr., “Four Noble Truths,” Encyclopedia Britannica, http://www.britannica.com/EBchecked/topic/214989/Four-Noble-Truths (accessed May 20, 2008).
[3] The teachings on the five khandhas: form (body), feelings, perceptions, thoughts, and consciousness, give us the tools to relieve suffering.
[4] Geoffrey DeGraff (a.k.a. Thanissaro Bhikkhu), “Life Isn’t Just Suffering,” rev. 2005, http://www. thaiexotictreasures.com/suffering.html (accessed May 20, 2008).
[5] Jos Slabbert, “How to Deal with Suffering,” http://www.taoism.net/theway/suffer.htm (accessed May 26, 2008).
[6] Jos Slabbert, on Lao-tzu, Tao Te Ching, Chapter 1, “attachment brings sorrow, but joy too,” http://www.taoism.net/theway/suffer.htm (accessed May 20, 2008).
[7] Jos Slabbert, on Lao-tzu, Tao Te Ching, Chapter 16 “the source is our true self,” http://www taoism. net/theway/suffer.htm (accessed May 20, 2008).
[8] Jos Slabbert, on Lao-tzu, Tao Te Ching, Chapter 23 “a willingness and courage to face reality is the only way to deal with suffering, especially when the suffering is inevitable. It is when you “embody” the Tao, accepting the inevitable, that you can face suffering with true equanimity,” http://www.taoism.net/ theway/suffer.htm (accessed May 28, 2008).
[9] Personal communication with Thomas In-sing Leung, Ph.D. (University of Hawai’i), Director of the Culture Regeneration Research Society in Vancouver, B.C. He was on the faculty of Regent College, University of British Columbia, and has served in several Chinese universities (Sichuan and Shandong) as Doctoral Dissertation Advisor.
[10] 2 Cor. 1:3-4 KJV, “Blessed be God, even the Father of our Lord Jesus Christ, the Father of mercies, and the God of all comfort, who comforteth us in all our tribulation, that we may be able to comfort them which are in any trouble, by the comfort wherewith we ourselves are comforted of God.”
[11] Thomas In-sing Leung, From Suffering to Hope [in Chinese], CD-ROM (Vancouver, BC: Culture Regeneration Research Society Productions Association, 2004).
[12] Paul T. P. Wong, “Chinese Positive Psychology,” Encyclopedia of Positive Psychology, ed. Shane J. Lopez (Malden, MA: Wiley-Blackwell Pub., 2009), 152.
[13] Jos Slabbert, “Body’s ‘intelligence’ refers to wisdom and compassion. It represents the intuitive, natural intelligence – the gut feeling of what is right – of someone living in harmony with the Tao,” http:// www.taoism.net/theway/suffer.htm (accessed May 28, 2008).
[14] Jos Slabbert, on Lao-tzu, Tao Te Ching, Chapter 18, http://www.taoism.net/theway/suffer.htm (accessed May 20, 2008).
[15] Kerry W. Bowman and Peter A. Singer, “Chinese Seniors’ Perspectives on End-of-Life Decisions,” Social Science and Medicine 53, no.4 (2001): 455-64.
[16] Paul T. P. Wong, “Chinese Positive Psychology,”152.
[17] Carl Ratner and Lu-mei Hui, “Theoretical and Methodological Problems in Cross-Cultural Psychology,” Journal for the Theory of Social Behaviour 33, no. 1 (2003): 72.
[18] Harry C. Triandis, Culture and Social Behavior (New York: McGraw-Hill, 1994), 161.
[19] Paul T. P. Wong, “Chinese Positive Psychology,” 152.
[20] Interview #12, Appendix.
[21] The Vinegar Tasters was mentioned in Benjamin Hoff’s book The Tao of Pooh (New York: E. P. Dutton, 1982), 2-7, http://en.wikipedia.org/wiki/Vinegar_tasters.with picture (acessed May 14, 2008).
[22] Donald S. Lopez, Jr., “Four Noble Truths,” Encyclopedia Britannica, http://www.britannica.com/EBchecked/topic/214989/Four-Noble-Truths (accessed May 20, 2008).
[23] Wei-ming Tu, Confucian Thought: Selfhood as Creative Transformation (Albany: State University of New York Press, 1985), 23.
[24] Benjamin Hoff, The Tao of Pooh (New York: E. P. Dutton, 1982), 6.
[25] Ming-dao Deng, Scholar Warrior: An Introduction to the Tao in Everyday Life (San Francisco: HarperSanFrancisco, 1990), 253.
[26] See story from Interview #6, Appendix.
[27] See story from Interview #12, Appendix.
[28] “Quality of Life” means different things to different people, as suggested by Matthew Edlund and Laurence Tancredi, “Quality of Life: An Ideological Critique,” Perspectives in Biology and Medicine 28, no. 4 (Summer 1985):591-607. This will be further discussed in Chapter 3 of this dissertation, page 91.
[29] Stanford Encyclopedia of Philosophy, “The Meaning of Life,” http://plato.stanford.edu/entries/life-meaning/#MeaMea (accessed May 14, 2008).
[30] Interview #10, Appendix.
[31] Mencius, “To die to achieve ren (compassion)” and “To lay down one’s life for a cause of 義 yi (righteousness)” in Mencius 6A: 10, trans. D.C. Lau (Harmondsworth: Penguin, 1970).
[32] Jos Slabbert on Lao-zi, Tao Te Ching, Chapter 154, “acceptance of the inevitable makes suffering bearable,” http://www.taoism.net/theway/suffer.htm (accessed May 20, 2008).
[33] Jos Slabbert on Lao-zi, Tao Te Ching, Chapter 74, http://www.taoism.net/theway/suffer.htm (accessed May 24, 2008).
[34] Mencius, “I would rather take dutifulness than life” in Mencius VI A: 10, 166.
[35] Ping-cheung Lo, “Confucian Values of Life and Death and Euthanasia,” Annual of the Society of Christian Ethics 19 (1999): 318.
[36] Ibid.
[37] Kantian philosophy has long cherished the value of individual autonomy, which emphasizes the freedom to decide on things that matter much to oneself. Some of its followers believe that human beings have the right to choose between life and death for themselves.
[38] Arthur Waley, trans. The Analectsof Confucius (New York: Everyman’s Library, 2001), 8.3.
[39] A paraphrase from the Classic of Poetry, one of the Five Classics (ancient Chinese books) used by Confucius and his followers as the basis of studies. Believed to be compiled or edited by Confucius himself. The others are Classic of Changes, Classic of Rites, Classic of History, and Spring and Autumn Annals.
[40] David Wong, “Comparative Philosophy – Chinese and Western,” rev. 2005 in Stanford Encyclopedia of Philosophy, http://plato.stanford.edu/entries/comparphil-chiwes (accessed May 24, 2008).
[41] Lo, “Confucian Values,” 322.
[42] Thomas P. Kasulis, Intimacy or Integrity: Philosophy and Cultural Difference (Honolulu: University of Hawai’i Press, 2002), 156.
[43] The Pali Canon is the primary sacred text in Buddhism, especially in the Theravada tradition.
[44] An arahant is a “worthy one” or “pure one,” an enlightened person who is not destined for further rebirth. It is a title reserved for Buddha and the highest level of his noble disciples.
[45] Damien Keown, “Buddhism and Suicide: The Case of Channa,” Journal of Buddhist Ethics, 3 (1996): 8-31.
[46] “Euthanasia: The Buddhist View,” BBC Religion & Ethics Forum, Feb. 24, 2004, http://www.bbc. co.uk/religion/religions/buddhism/buddhistethics/euthanasiasuicide.shtml (accessed May 24, 2008).
[47] Bhikku Dhammavihari, “Euthanasia: A Study in Relation to Original Theravaden Thinking,” presented at the Y2000 Global Conference on Buddhism, Singapore, June 3-4, 2000, http://www.metta.lk/ english/euthanasia.htm (accessed May 24, 2008).
[48] Chad Hansen, “Taoism,” Stanford Encyclopedia of Philosophy, rev. 2007. Simplicity (in Tao Te Ching, Chapter 37) and humility (Tao Te Ching, Chapter 7) are two other cardinal virtues in Taoism.
[49] According to Xinhua National News, these surveys have found a high percentage of people, from 95% (among medical workers) to 64.6% (among Beijing residents), in 2003 opting for “mercy killing” if they ever become terminally ill with intractable pain. Legal Daily, June 12, 2007 edition [in Chinese], http://www.news.xinhuanet.com/legal/2007-06/12/content_6230138.htm (accessed May 20, 2008).
[50] The March 6, 2006 edition of China Daily reported in an article “Local Experiments on Euthanasia Proposed” that a province-level hospital in North China’s Hebei Province each year would encounter one or two cases in which patients with terminal illness would ask for “mercy killing,” http://www.chinadaily.com.cn/english/doc/2006-03/06/content_527285.htm (accessed May 20, 2008).
[51] William David Solomon, “Double Effect,” in The Encyclopedia of Ethics, 2nd ed., ed. Lawrence C. Becker and Charlotte B. Becker (Florence, KY: Routledge Press, 2001), 418. The principle of “double effect” is often invoked to explain the permissibility of an action that causes a serious harm, such as the death of a human being, as a side effect of promoting some good end, such as pain relief.
CHAPTER 3: Western Philosophical Perspectives on the Meaning of Life
My friend Feng and I were huffing and puffing as we climbed the stairs. There was no lift in this seven-story apartment building. The staircase was dark. Garbage was found in every corner. A rancid smell was in the air. Multiple electric meters were hanging from the wall and wires were crisscrossing everywhere. Almost every household had a stainless steel burglar-proof gate in front of their wooden door. The sound of traffic downstairs got more muffled as we climbed. Finally, we arrived at Mr. Zhang’s apartment on the seventh floor! [1] We were greeted by a red placard pasted above the door – saying “God is Love” – written in Chinese with black ink. We rang the doorbell.
A burly-set woman in her forties came to the door. That was Ai Yi, Mr. Zhang’s wife. We got introduced. Feng had told me earlier that this was Mr. Zhang’s second marriage, with the first one ending in divorce, and leaving him with three boys and one girl. Ai Yi herself had a 22-year-old son from a previous marriage, now living with his father.
We were greeted warmly and invited into the apartment, which was small but homely. Newspaper was neatly folded on the side table. On the wall next to the dining table was a wooden cross. There were fresh flowers in a vase on top of the table. Sitting in front of the small television set was Mr. Zhang. He looked emaciated and cachectic. His hair was unruly, mostly silvery white, and thinned out at the top. Feng had informed me earlier that Mr. Zhang was dying from lung cancer, but the seriousness of his medical condition had not been disclosed to him as yet.
“Welcome, Feng; and you, my friend,” Mr. Zhang said, as he tried to get up from the sofa.
“Thank you for allowing us to visit you and Ai Yi. How are you?” I replied.
“This body of mine is not much good now. It is rusting away.”
“I guess none of us is getting any younger.”
“How did you find the stairs? Did you…” he enquired, but had to stop to catch his breath.
“The stairs were rough for me. What about you?”
“I get tired and short of breath easily. The doctor said my lungs are filled with fluid. So, I hardly go out anymore. I wanted to find an apartment on the lower floor, but the rent was horrendous. I wish there were lift, but apparently they are not mandatory unless the building is more than seven stories high.”
“It must be rough staying home all the time.”
“Ai Yi took me out sometimes. She would carry me on her back to get me downstairs.”
“That’s awfully nice of you,” I said to Ai Yi, as she sat down on the sofa next to Mr. Zhang.
“She used to take me out on outings in the country on her motorcycle. I enjoy taking those rides with her to new places and view the beautiful scenery along the way. The ride means relaxation and freedom to me. I cannot begin to explain how relaxed I felt when we were cruising down the country road, with the wind caressing my hair, and the breeze brushing against my face on a warm sunny day. The ride helps me to clear my mind of worries and irritations, allows me to think creatively, and gives us quality time together. It also gives me a sense of freedom, because I feel that I can still go anywhere, physically or mentally. It makes me feel that everything is going my way, and that my goals are attainable after all,” Mr. Zhang said this with excitement and wonderment in his eyes, as he put his arm on Ai Yi’s shoulders.
“That’s wonderful!” I replied.
“When my own family cast me out in my hour of need, Ai Yi took me in. Even my own children rejected my pleas for help. They slapped on us many unfair demands before they would even consider lifting a finger to help us. I guess I was too kind-hearted a father, spoiling my children and failing to bring them up properly. This is one regret I shall take with me to my grave.”
“How about making reconciliation with them?” I enquired.
“It’s not much use. Like their mother, they are really prejudiced against Ai Yi.”
“What do you think, Ai Yi?” I said, turning to Ai Yi.
“It’ll be good for Dad to be reconciled with his children. There’s been a lot of misunderstanding. I’ll do what I can to smoothen it out,” said Ai Yi.
“It’s mighty noble of you.”
“Ai Yi is God-sent,” Mr. Zhang interjected. “I love her more than my own family. I would have killed myself in despair if it wasn’t for her. She is my reason for living. I wish I could provide more for her, but she is easily contented. She says she’ll be happy to be with me through thick and thin. I love to be with her. That’s one hope I cling to when everything looks dismal and grey.”
“That’s great!”
“I thank God every day for His blessings. God is good. Since my retirement, things were tough, especially with money, but God did provide enough for our needs. We have learned to rely on His faithfulness, and on His grace which is more than sufficient for me. I’ve missed out a lot on the peace and harmony that many have found in their family life, but I can now count on the joy of sharing a home with Ai Yi, and the peace of a heavenly home yet to come.”
Mr. Zhang passed away a few months later, in March 2008. I visited Ai Yi in October the same year when I returned to China. She was still grieving, but had a lot of sweet memories to cherish. She looked forward to the day when she would join her husband in that heavenly home. Both of them had found meaning in their lives – their Christian faith, their authentic self in choosing their own lives to lead, the affirmation of being loved, and the assurance of peace and joy in a place called home, on this earth and for all eternity.
In my field work in China, I have found many Chinese whose lives are heavily influenced by or exemplify Christian theology or post-Christian era Western philosophies. Mr. Zhang was one of several Christians I interviewed. His meaning of life was quite different from that of Ms. Zeng, whose story was told in the previous chapter. [2] Ms. Zeng was not religious. She was more concerned about living life to the fullest. Quality of life ranked high among her values. In other words, she would be the typical “heroine” in Camus’ narrative.[3] Her desire to make her own decisions would also make her a central character in the personal narrative of Nietzsche or Sartre. In the two stories of Mr. Zhang and Ms. Zeng, we find two very different people in contemporary China: Mr. Zhang being heavily influenced by Western theology (Christian theology), and Ms. Zeng by Western philosophy. Indeed, Chinese and Western traditions interact and enrich one another.[4] In exploring such an elusive concept as “meaning of life,” each tradition can have something insightful to say and incorporate something of what the other tradition has to say. This fruitful interaction and mutual influence would go a long way in helping us understand the human stories being told in China, and in the West too. In this chapter, we will examine, philosophically and existentially, Western perspectives on the meaning of life, including faith, freedom, love, and hope. In doing so, we can reflect on our most deeply entrenched and otherwise unquestioned agendas and assumptions of our own tradition, whether it is Chinese or Western.
True-World Philosophy
True-world philosophy originates from the dialogues of Plato. Plato’s way of giving meaning to life has dominated virtually the entire history of Western thought and feeling, exerting its influence not only on Christianity, but also in disguised forms in the post-Christian era.
As Socrates’ student, Plato believed in the immortality of the soul and provided an explanation for the suffering soul. “The soul,” being the animating source of all actions “is immortal,” says Socrates. The soul is the “uncaused” cause of action, because it can freely decide. For instance, nothing compels us to act when we freely decide to do something. Thus, Socrates argues, the soul is immortal, because it can neither come into, nor go out of, existence. It cannot come into existence because then it would have to have, after all, a cause. And it cannot go out of existence because the only way something can cease to exist is through the removal of its originating and sustaining cause. This soul originally received its “true nourishment” from “the rim of the heavens.” [5] Reason, according to Plato, is “the soul’s pilot,” exerting command over physical desires which Plato refers to as “appetite.” [6] A rapacious “appetite” can cause spiritual sickness and suffering in the soul. On account of the struggle to control physical desires, some souls had “their wings broken.” No longer able to fly, they fell to earth where they became incarnate and entered into material bodies, where they were condemned to repeated re-incarnations in bodily form, with its current position in the order of things being determined by the merit or otherwise of its previous life. However, in time, with the pursuit of knowledge, knowledge of the “Forms,” the soul can return to the heavens. In many ways, Plato’s philosophy (developing around 4th Century BC) may have influenced Buddhism (developing around 3rd Century BC), which also believes in desires causing suffering, karma and re-incarnations of the soul until enlightenment is achieved.
Just what are these Forms? In The Republic, Plato divides reality into two worlds: the world of Forms (or being) and the world of becoming.[7] The world of Forms is the true world, an invisible world, but nonetheless absolutely real, which Plato calls the world of unchanging “being.” Forms are truly the things they are, whereas things in this world of becoming, which is a world of senses, are only approximate copies of their original Forms in the world of true being. This dichotomy is the heart of Plato’s philosophy. When the material body is withering fast and when the soul feels imprisoned within that earthly body, one is reminded of a certain “bitter-sweetness;” bitter because the sensation and feeling are reminders of the powerlessness and suffering associated with an earthly body, and sweetness because with hope, a return to the true home in “the rim of the heavens” can now be anticipated. In other words, knowing or remembering the true Form (in the form of a “heavenly” body or dwelling) brings comfort and peace to the suffering souls in this world who yearn for a return to the heavens.
Since the Forms are the standards, ideals or perfect examples of which things in the everyday world are at best imperfect copies, so the Forms of the courageous, the just, the good, and the wise are the virtues of courage, justice, goodness and wisdom. In fact, it was Aristotle, Plato’s student, who took this concept of virtue one step further as he developed his doctrine of the Mean.[8] According to Aristotle, a virtue can be seen as the mean of two extremes: deficiency and excess. For instance, the virtue of courage can be recognized as the mean between cowardice (on the deficiency side) and recklessness (on the excess side). Even though Aristotle did not elaborate on hope as a virtue, hope can be seen as the mean between despair and presumptuousness.
Thus, in summary, Plato’s “grand narrative” that gives meaning to life has three parts. It is a story of (1) initial grace – dwelling in a heaven called home, the right place; (2) a fall from grace – to a place of alienation and exile; and (3) redemption – homecoming, a return of the soul to the place from whence it came. According to Julian Young, Plato’s narrative further demonstrates that (a) the character of life’s goal or meaning is determined by its past; (b) we are sometimes vulnerable to exile and alienation, an existential concern; (c) it is our own fault that we are here in our present conditions of sickness and suffering, since the fall is the result of our failure to control our “appetite;” and (d) we should know and practice the virtues if we are to achieve our goal in life.[9]
Evidently, the influence of Plato’s grand narrative on Christianity is immense, even though there is no omnipotent creator-God in Plato, and there is nothing in Plato that corresponds to the self-sacrifice of God to save humankind. Yet, Christianity is basically a version of Platonism, of the true-world or true-home view of reality. There is the same immortal, immaterial soul which figures in Plato’s three-part story of grace, fall from grace, and redemption. In both stories, there is the same metaphysical dichotomy between the natural and the supernatural worlds, between earth and heaven, between alienation and homecoming. In both stories, the fall is our own fault. Thus, Plato’s narrative achieved virtually complete domination over Western thinking from about the beginning of the 4th Century BC until well into the 18th Century AD. During this time, the question of the meaning of life was a non-issue, because the answer was so obvious, as offered by Christianity’s version of Platonism.
It was Immanuel Kant (1724-1804) who saw that the old Platonic-Christian true-world grand narrative had become problematic. With the 18th Century Enlightenment, the birth and success of experimental science started to challenge traditional Christianity. The basic character of the Enlightenment was a tremendous optimism about the power of human reason. No longer was knowledge a dispensation from God, as it had been in the Middle Ages, but rather, it was humanity’s own achievement, the product of human reasoning based on careful observation of the visible world. God and the soul faded into insignificance. Plato’s world of Forms, the supernatural, immaterial, and transcendent true world of being, turned out to be nothing but a myth to the rationalists.
Immanuel Kant, being a rationalist as well as a religious conservative, attempted to rescue the traditional religious belief by distinguishing a “world of sense” from the true “transcendental” world.[10] He maintained that there is still a supernatural true world which feeds us all the input that is filtered through our human lenses, giving us an apparent experience of the true world. He suggested that our kind of space, time, and “thing-ness” are only apparent forms of the true world. For instance, if we are wearing green-tinted sunglasses, then all the things we see will appear green, even though, in reality, only some are. For Immanuel Kant, the space-time world of nature that is described by science is only an apparent world of phenomena, as related to our own intuition,[11] whereas the supernatural world is the true world, the ultimately real domain of the “thing in itself” which is absolutely unknowable by our human mind or physical senses except by faith, a faith in a “supremely wise cause” that is the “archetype of all reason.”[12] This faith provides the ground for our existence, and the basis of hope.
In addition, as a rationalist, Immanuel Kant claims that Christian belief is “rational.” His argument runs roughly like this: (1) when we are committed to morality, we believe in punishment and reward; (2) but since many wicked prosper and the good die young, there must be an afterlife when punishment and reward are doled out by a just God; and (3) since getting one’s just treatment in an afterlife must mean that one has to be around in that life, there is reason to believe that all souls are immortal. Given this “rational” Christian belief of a just God, an immortal soul, and an afterlife, there is meaning to our lives.
Arthur Schopenhauer (1788-1860), often called a pessimist and nihilist, widely criticized this Kantian attempt to save Christianity. While he fully accepts Immanuel Kant’s distinction of the two worlds (one of appearance and one of ultimate reality), Arthur Schopenhauer argues that the sensory world of appearance is so overwhelmingly full of cruelty and suffering that it is hard for him to see the latter world, the supernatural world, to be inhabited by the Christian God of love. Furthermore, he disagrees with Immanuel Kant regarding the unknowabiliity of the “thing in itself.” Arthur Schopenhauer points out that knowledge (including knowledge of God, if there is one), rather than being the product of the mind or physical senses, can be grounded in many subtle ways in human experience. He argues that an account of things through personal experience can certainly help one to know the “thing in itself.”[13]
Despite such objections, Arthur Schopenhauer still clings to the true world of the “thing in itself.” He does endorse the Christian idea that this earthly world is a “veil of tears” from which we need other-worldly salvation. However, he believes that this salvation is brought about, not by God, but by the transcendence of “individuality” or the self. It seems that the difference between Arthur Schopenhauer and Christianity is that his true world is not populated by God and angels, but is the atheistic true world of Buddhism, where the absolute or ultimate “thing in itself” is the will (or desire) to live. Instead of interpreting the “thing in itself” as good and blessed, Arthur Schopenhauer interprets it as “absolutely reprehensible”[14] In this atheistic true world, Arthur Schopenhauer believes that redemption can come only if one would let go of one’s will or desire. That is why Arthur Schopenhauer’s philosophy has been called “European Buddhism” in Friedrich Nietzsche’s later writing.[15] The goal and meaning of life, according to Arthur Schopenhauer, is letting go of one’s will or desire so as to arrive at a deep tranquility and calmness of the spirit, an eternal bliss that Buddhists call Nirvana.[16]
Friedrich Nietzsche (1844 –1900), in his early writing (The Birth of Tragedy), tells us that we all yearn and hope for something that would (1) provide meaning for our sorrow and (2) help us to transcend the tragedy of life. [17] The question Friedrich Nietzsche focuses on with regard to Greek tragedy is the nature of the “tragic effect,” a question that has puzzled philosophers since Aristotle: “Why is it that we willingly subject ourselves to the sight of the catastrophic, the destruction of not just human beings, but in many respects the finest examples of what humanity has to offer?” Is there presumably some kind of satisfaction derived from this? When describing this “tragic effect,” Friedrich Nietzsche uses the same word as Immanuel Kant – the feeling of “the sublime” – to describe the feeling of becoming alive to one’s super-phenomenal nature as one temporarily escapes from the bitterness and torments of existence as an individual experiencing the phenomenon of suffering, and is reminded of “another existence and a higher pleasure for which the tragic hero prepared himself by means of his destruction.”[18] Here is Friedrich Nietzsche’s answer: whereas Apollonian art teaches us to take delight in the phenomenal world, Dionysian art “teaches us that we are to seek joy not in the phenomena but behind them.”[19] Friedrich Nietzsche offers us an alternative explanation of suffering that is different from Arthur Schopenhauer’s.[20] Friedrich Nietzsche suggests that, in order to escape the pain of life as individuals, we must go “beyond good and evil” as we identify with the author-creator of the world, the source of existence. Friedrich Nietzsche believes that the source of all existence is to be conceived neither as the Good who provides for us nor as the Bad who doles out suffering, but rather as “an entirely reckless and amoral artist-god” who will from time to time destroy the sandcastle-worlds it has built and construct new ones instead.
Later on in his writing, Friedrich Nietzsche says of Arthur Schopenhauer, “Against the theory that the ‘thing in itself’ must necessarily be good, blessed, true and one, Arthur Schopenhauer’s interpretation of the ‘in-itself’ as will was an essential step; but he did not understand how to deify this will; he remained entangled in the moral-Christian ideal…seeing it as bad, stupid, and absolutely reprehensible.” [21]
Like Arthur Schopenhauer, the early Friedrich Nietzsche was also a European Buddhist, believing that “individuality is the source of all suffering,”[22] and that salvation comes from the transcendence of this “individuality.” In his Birth of Tragedy, Friedrich Nietzsche explained that suffering is a disjunction between subjective wants and objective findings. Hence, according to Friedrich Nietzsche, if one would just let go of one’s subjective wants, and go beyond (or transcend) individuality, there can be no more suffering to the individual.
Georg Hegel (1770-1831), in a refreshing change, looks into the future of this world for peace and harmony, rather than a super-natural world for redemption. For Georg Hegel, who rejects the Kantian true world of Christianity, the true world is still maintained, though relocated, from a supposed other world into the future of this world. The distinction between nature and super-nature is re-interpreted as a distinction between present and future.
Georg Hegel emphasizes co-operation within a community, showing that we are united together, with one another and with nature. [23] In Georg Hegel’s thesis, the “I” is the ultimate reality. The “I” is essentially “something which is only for others.”[24] In Jean-Paul Sartre’s rephrasing of this thought, it means that the other holds the secret of my being, as I come to know myself and the world. For instance, if I want to be confident of my independent existence as a loving husband and kind father, I can only be certain of possessing this nature if my wife and children accord me the recognition.
To Georg Hegel, the meaning of life consists of an attainment of a true world, a state of apocalyptic peace and harmony at the end of history, when there is no more alienation between you and me. As with Christianity, the meaning of life, in Hegelian terms, is the attainment of the “city of God.” The only difference is that it is located not in the sky but on the (future) earth. In Friedrich Nietzsche’s language, what Georg Hegel offers is a kind of “metaphysical comfort” for the alienation of the present, a hope that one day, as history unfolds toward a final utopia, alienation will be overcome and everyone will live in peace and harmony.[25] To Georg Hegel, a happy life is a life of harmonious co-operation, grounded in the fact that every individual recognizes his or her true self in the “ethical substance” (or ethos) of a people or community.
Georg Hegel also believes that there is a general will that belongs, fully and equally, to all individuals. It is a universal essence of humanity equally present in all social classes.
By fulfilling one’s own special function, the collective will can be fulfilled, just as members of a team contribute to the success of the whole by fulfilling their own, individual role or utility.[26] Georg Hegel believes that this “utility” of functions, this practical, instrumental consciousness, is a criterion of existence. Nothing exists unless it has utility. It is this utility that helps to shape the general will, overcomes alienation, and diminishes the subject-object class distinction. One example of this general will is the revolutionary spirit that brought about the French Revolution to overthrow the oppressive “bourgeois” society. A new world dawns with the unfolding of history toward a better and more progressive society. At least, that is how Georg Hegel saw it. This also reminds us of the Communist Revolution in China as well as the Chinese beliefs in collectivism and utility of efforts. It echoes what Ellen Marshall says about hope. “Hope is virtuous when it orients us toward the flourishing whole, and this requires me to see my well-being as wrapped up with yours.”[27]
When Friedrich Nietzsche reported in 1882 that “God is dead,” [28] he did not mean merely the God of traditional Christianity. He meant rather that performs the function in human life that was once performed by the God of traditional Christianity. He was pointing out the truth that, sociologically, the Western culture has ceased to be a religious culture. A religion is anything that postulates or promises a true world. In this sense, Christianity and ‘European Buddhism’ count as religions; so do Hegelianism and Marxism.
Whereas Georg Hegel sees history as embodied in human activity in general, Karl Marx (1818 – 1883) sees history as embodied in just one kind of activity: economic activity – activity concerned with the production and ownership of material wealth. To Karl Marx, economics provides the foundation of history; everything else – art, religion, politics, law – is mere “superstructure,” the foam on top of the beer. Religion, Karl Marx famously said, is the “opium of the masses.” Just like Georg Hegel, Karl Marx posits a paradise, a utopia, a true world whose anticipated arrival will herald the “end of history.” Like Georg Hegel, therefore, Karl Marx is also a covert true-world philosopher in disguise. Like Georg Hegel, Karl Marx also translates the duality between nature and super-nature into a duality between present and future, to reproduce the meaning-giving structure of Platonism and Christianity within the one world of nature. When Friedrich Nietzsche pronounced that “God is dead,” there appeared to have no more version of the true-world answer to the question of the meaning of life that would seem to merit belief. Without the “true world” or religion as the ground for hope, humanity entered into a world of nihilism where traditional values and beliefs are unfounded and human existence is often considered senseless and useless.
Continental Philosophy
From the end of the 19th Century to the present, the works of philosophers abound to respond to this question of what can be said about the meaning of life in light of the “death of God.” These include writings from the later Friedrich Nietzsche, Jean-Paul Sartre, Martin Heidegger, Albert Camus and others. Their thoughts constitute collectively the “Continental philosophy,” [29] which generally opposes the grand narratives of “True-world philosophy.” Continental philosophy begins with the recognition that not only the Christian God but also all these “shadows of God” [30] which include the “true world” of Georg Hegel and Karl Marx, are simply mirages, “anthropomorphic” projections, wishful thoughts that have no basis in reality. The death of God, Friedrich Nietzsche holds, results in the depreciation of values that have been regarded hitherto as the “highest values.”[31] They no longer grip us, and they are no longer able to give direction and meaning to our lives. A value vacuum comes into being, which Friedrich Nietzsche calls “nihilism.” In such a value vacuum, Friedrich Nietzsche asks, “If reality is chaos, how can life be worth living or meaningful?”[32] Friedrich Nietzsche’s answer is that a person can still find life meaningful in stories, in personal stories.
Stories can create meaning, Friedrich Nietzsche suggests. Every true-world philosopher is, in one way or another, a story-teller. Every true-world philosophy from Plato onwards, in one way or another, tells a story of “the soul’s journey” that has universal meaning to everyone. What about personal stories? In order to create personal meaning in our lives, we must, Friedrich Nietzsche says, become the hero or heroine of our lives. Here, it does not necessarily mean “performer of heroic deeds.” It simply means central character, just like the hero or heroine in a novel. Friedrich Nietzsche suggests stepping back to view our own lives, and create a personal meaning in it. He wants us to think visually here. If one is very close to something – say a mountain – all one sees are its details, all the trees in the foreground. But if we step back and allow some distance in between, we will see the overall shape of the mountain. The sameis true with regard to our lives, Friedrich Nietzsche says. If we allow some distance to view our life as if from its end, we may be able to see the “big picture” with ourselves being the heroes of a well-constructed novel, and a meaningful one at that.
Friedrich Nietzsche calls this becoming a “poet of one’s life” to draw attention to the idea that living a meaningful life is living it as though one is in the process of creating a fine work of art. This is how one grasps the overall character, the personal narrative, of one’s life. To become heroes or heroines, Friedrich Nietzsche says, we need to learn from artists “the art of viewing ourselves…from a distance and – as it were, simplified and transfigured – the art of staging and watching ourselves…Without this, we would be nothing but foreground and live entirely in the spell of that perspective which makes what is closest at hand…appear as if it were vast, and reality itself.” [33] In many ways, our suffering is seen in the foreground and appears as if it were reality itself, but if we would only step back, or see it from a later time, we would see a different picture altogether.
This personal narrative is also very much like the earlier mentioned Platonic or Christian grand narrative, in terms of knowing the past, realizing the present, and projecting into the future. It tells one of three things: (1) one’s history up to now; (2) one’s present condition; and (3) a projection of one’s life into the future. To know the story of one’s past and present is to know who one is – one’s identity. Knowing one’s identity will give meaning and purpose to one’s life, and sustain one in living through chaos and adversities, confident in one’s destiny in the future, just as hope “orients us toward the flourishing whole, empowers us to labor on its behalf, and sustains us in the meantime.” [34]
Nietzsche believes that human beings have the opportunity to make major decisions at various branching points in their lives. Mr. Zhang chose to live with hope in his heart though his suffering was getting unbearable.[35] Ms. Zeng, on the contrary, would choose suicide to free herself from pain and suffering.[36] No matter how they choose, it would be up to them to choose their own personal stories. Friedrich Nietzsche contends that we create who we are. His notion of “existence before essence” is the central principle of existentialism. It is for this reason that he is often regarded as the first existentialist.
Friedrich Nietzsche also believes in redemption. It is just as important to him that a personal narrative should be redemptive as that a grand narrative should be so.[37] A redemptive state is the final state that brings history to an end, a state that makes sense of, and makes up for, the pain and suffering that have preceded it. Not all personal narratives are redemptive. Some are self-loathing and filled with despair, where the stories constructed depict the self as victim or villain rather than hero. In a redemptive personal narrative, one must construct a self that one desires and esteems, finding a meaning in one’s life. To do so, says Friedrich Nietzsche, we must be able to see a “personal providence” in things, when we see how palpably always everything that happens to us turns out for the best. Every day and every hour, life seems to have no other wish than to prove this proposition again and again. Whatever it is…the loss of a friend, sickness…failure, it proves to be something that must not be missing; it has a profound significance and use precisely for us. [38]
How can one achieve this state of mind? Friedrich Nietzsche suggests reminiscence of the past [39] to bring out the major achievements of one’s life, so that the petty and the inconsequential will disappear in the process.[40] Friedrich Nietzsche calls it creative amnesia. He explains it this way, “Mirabeau had no memory for the vile actions done to him. He was unable to forgive simply because he forgot.” [41] In modern psychological terms, this may sound very much like the half-full versus half-empty glass analogy.
This concept of personal narrative has laid the groundwork for current narrative therapy. Reminiscence of the past may help to diminish the pain and suffering of the present, and stir up “an overflowing energy that is pregnant with future.”[42] This energy helps to drive the goal that is created by a sick person, and may well sustain her/him in living through a terminal illness. That is the dawning of hope.
In contrast, Martin Heidegger (1889-1976)proposes that meaning of life is not freely chosen but discovered in conjunction with heritage and the particular historical situation or socio-cultural context. Martin Heidegger’s crucial thought is that heritage is not something we choose. Rather, we are born into it. As we grow to adulthood – always, of course, within a particular culture – we find ourselves already in possession of a pantheon of hero-figures and the values they personify.[43] These role models or exemplary figures can tell us how to live. Of course, each person can still make choices that are different from what that particular culture or community expects. Thus, each person can have a different meaning of life as one focuses on both a united communal goal and one’s autonomy.
Jean-Paul Sartre (1905-1980) disagrees with Martin Heidegger. Jean-Paul Sartre contends that the only real meaning in life lies in being authentic to one’s true self. When we find ourselves not accepting our true self but the self that is communally constructed by heritage, then life is no longer meaningful. According to Jean-Paul Sartre, I am who I choose to be. He rejects the theory of psychological determinism which holds that the kind of person that I am, including all my future choices and actions, is completely determined by the totality of physical and cultural facts about me: my biology, my heritage, my history, my experience, etc.
Jean-Paul Sartre maintains that we not only choose our identities but our world as well. We see the world through our own values that give us meaning. Since I choose my values – cannot but choose them, according to Jean-Paul Sartre – I in fact create my own world. When Mr. Li was afflicted with colon cancer, [44] he could interpret this event as a horrible experience, making him a victim, or he could interpret it as an edifying experience, a positive experience, which prompted him to say, “I hope to be a good example to them (my children) by facing my problem head on and not running away from it. If I simply stop fighting and kill myself, what kind of example am I setting for my children?” In every case, Jean-Paul Sartre claims that I am the author of my own misfortune and am solely responsible for the consequences. Since the world is my own creation, I have no excuse to shirk responsibility. Jean-Paul Sartre’s doctrine of freedom and responsibility clearly owes a great deal to Friedrich Nietzsche’s ideas on self-creation.
When Albert Camus (1913-1960) writes at the beginning of The Myth of Sisyphus, “There is but one truly serious philosophical problem…and that is suicide…judging whether life is or is not worth living,”[45]the question of suicide is just a dramatic way of posing the question of life’s worth or value. Albert Camus points out that humanity has a need to believe either in God or in a miraculous event at the end of time. When this need confronts the evident failure of reality to provide such meaning, life becomes absurd and is filled with alienation, estrangement, and disengagement. All values are lost and a “deadly weariness” sets in, resulting in a “longing for death.”[46] Albert Camus’ central task is to reject this inference, to show that even if one does not believe in God, suicide is not legitimate. It is not legitimate because, as Albert Camus claims, “it is possible to live and create in the very midst of the desert.”[47] In fact, Albert Camus aims to show that life can be lived splendidly even if it is absurd without meaning.[48] He maintains that it is possible for us to continue living just because our human nature impels us. It is in our nature to take life as it is, no matter how arduous the journey may be. We should simply accept life’s absurdity and live a splendid life with courage, integrity, perseverance and dignity. Albert Camus advises us to enjoy the present experiences of life’s journey and forget the destination. He contends that life is “not to be built up but to be burned up.” [49] Albert Camus’ hero or heroine lives in the present. Ms. Zeng was prepared to live her life to the fullest.[50] She used to be wrapped up in her business concern, but since she was diagnosed to have metastatic lymphoma, she learned to live in the present, becoming alive to the extraordinariness of the ordinary. “Life is filled with such wonderment and awe. I hope to spend more time with my husband and with my children…I hope to work creatively as a hair stylist as long as I am able to. I hope to continue gardening and watch in awe the flowers bloom after I plant the seeds. They say cats have nine lives. I only have one. Might as well enjoy the time I have now.”[51] Albert Camus contends that anticipation of the future kills the joys of the present. There is truth in that. Arthur Schopenhauer has a similar observation when he writes, “(People live) in the expectation of better things…On the other hand, the present is accepted only for the time being, is set at naught, and looked upon merely as the path to the goal. Thus when at the end of their lives most men look back, they will find that they have lived throughout ad interim; they will be surprised to see that the very thing they have allowed to slip by unappreciated and unenjoyed was just their life, precisely that in the expectation of which they had lived.” [52]
Quality of Life
Like meaning of life, quality of life is an elusive concept that refers to the significance of meaning, the extent to which something matters in life. It has been defined as an “overall sense of well-being with a strong relation to a person’s health perceptions and ability to function. On a larger scale, quality of life can be viewed as including all aspects of community life that have a direct and quantifiable influence on the physical and mental health of its members.”[53] It is a descriptive term that refers to people’s state of physical, emotional, and social well being, as well as their ability to function in the ordinary tasks of living. Physically, one can be well nourished and healthy or one can be sapped bone dry and dying. One’s emotional state may be positive (filled with pleasure or delight) or negative (experiencing overwhelming stress or worry). Social relationships can be edifying or destructive, resulting in either intimacy or isolation. What is missing in this definition is the spiritual state, in which one can be content and peaceful, or perturbed and bitter.
Quality of life varies with individual value system, depending on the meaning one attaches to life. Thus, it is virtually impossible to predict the quality of life in any one individual, since the combination of attributes that leads tocontentmentvaries among different individuals.
Unlike standard of living, quality of life is not a tangible concept that can be easily measured. Anna Donald, an epidemiologist at University College, London, England, proposes that quality of life can be measured by the subjects themselves (such as level of pain or distress felt) or by observers, using measures of objective functioning in the ordinary tasks of living. [54] She cautions that it is important to cover both subjective and objective aspects and not to infer the quality of life from single scales.
Quality of life has different meanings for different users. Matthew Edlund and Laurence Tancredi have proposed five views of quality of life (QoL) based on different ideologies: (1) the self-fulfillment view, (2) the return to normality view, (3) the social utility view, (4) the rational-man view, and (5) the individualistic view. They suggest that to understand the use of the phrase (QoL) one must understand the personal meaning of the user. [55] Firstly, some users see QoL as the fulfillment of personal goals (or self-actualization). Secondly, some see it as the ability to lead a “normal life;” or thirdly, a “socially useful life,” when a person is able to function as a useful member of family and society (being employed and fulfilling the many expected socially defined roles). The fourth meaning, to the rational man, may suggest justice and equality as important values in his assessment of QoL. Fifthly, it is in the individualistic view of QoL that subjectivism reigns supreme. Here, QoL is what each individual defines it to be. Each individual will choose her/his own meaning(s) of life, rather than following the social values of the general community, culture or heritage. This conflict is especially stark around the issue of suicide: even if individuals come to the conclusion that life is simply not worth living and have numerous rational justifications for their view and their decision on Physician Assisted Suicide, societal mechanisms reflecting the general will may go to great lengths to refuse them the exercise of this option.
Quality of life should be considered not just in the corporeal realm, but also in the spiritual realm. The terminally ill believer may find, in the midst of suffering, one final opportunity to bear witness to her/his faith by showing others how to die well.It is in the spiritual realm that the quality of life can really shine. This final opportunity for the terminally ill person to bear witness of her/his faith in facing death should be facilitated by the caring communities. John Dunlop states:
Quality issues help us determine if we should use aggressive measures to prolong that life. When preserving the quality of life, rather than prolonging that life, is the goal, the result is a commitment to provide loving support and comfort to the patient.[56]
Search for Existential Meaning
For anyone who questions life and wonders if it has any meaning or value, Viktor Frankl’s book Man’s Search for Meaning provides much insight to answering this question. This is his reason for writing his life-affirming book:
“I had wanted simply to convey to the reader by way of concrete example that life holds a potential meaning under any conditions, even the most miserable ones. And I thought that if the point were demonstrated in a situation as extreme as that in a concentration camp, my book might gain a hearing. I therefore felt responsible for writing down what I had gone through, for I thought it might be helpful to people who are prone to despair.” [57]
In his book, Viktor Frankl chronicles his experience as a long-time prisoner in a bestial concentration camp with an entrance that reminds us of Dante Alighieri’s inscription on the entrance to Hell: “Abandon all hope ye who enter here.”

The entrance to the feared death camp of Auschwitz, home to author-psychiatrist Viktor Frankl, as prisoner of conscience of the Third Reich
Viktor Frankl found himself stripped to naked existence. His father, mother, brother, and his wife died in camps or were sent to gas ovens, so that, excepting for his sister, his entire family perished in these camps. How could he – every possession lost, every value destroyed, suffering from hunger, cold and brutality, hourly expecting extermination – how could he find life worth preserving? No wonder some prisoners simply gave up living. In despair, they refused to get up in the morning and go to work. They stayed in their huts, and lay on straw wet with urine and feces. Nothing could change their minds or their behavior. In the next forty-eight hours or so, it was evident that these prisoners were slowly dying.[58]
Viktor Frankl contends that people need a reason for living. He clearly saw that it was those who had nothing to live for who died quickest in the concentration camp. Viktor Frankl believes that when life is no longer meaningful, there is no more reason for living. On the other hand, prisoners who had found their lives meaningful would say yes to life despite the most sordid conditions of existence.
Viktor Frankl also contends that human beings are not only “capable of changing the world for the better if possible,” but also “changing themselves for the better if necessary,”[59] especially when the world cannot be changed. “Just think of an incurable disease such as inoperable cancer. We are challenged to change ourselves.”[60] We have the capacity to creatively turn life’s negative aspects into something positive or constructive. This can be done by discovering meaning in our lives.[61] Fundamentally, therefore, any person can, even under such (bestial) circumstances, decide what shall become of her/him – mentally and spiritually. One may retain one’s human dignity even in a concentration camp. “We have come to know man as he really is. After all, man is that being who invented the gas chambers of Auschwitz; however, he is also that being who entered those gas chambers upright, with the Lord’s prayer or the Shema Yisrael on his lips.”[62] Faith is a significant reason for living. “The prisoner who had lost faith in the future – his future – was doomed. With his loss of belief in the future, he also lost his spiritual hold; he let himself decline and became subject to mental and physical decay.”[63]
Viktor Frankl contends that meaning cannot be given; otherwise it would amount to moralizing. Meaning of life has to be found by each person. It differs from one person to another, and from moment to moment. Thus it is impossible to define the meaning of life in a general way. Questions about the meaning of life can never be answered by sweeping statements. ‘Life’ does not mean something vague, but something very real and concrete, just as life’s tasks are also very real and concrete. They form one’s destiny, which is different and unique for each individual. No one person and no destiny can be compared with any other person or any other destiny. No situation repeats itself, and each situation calls for a different response. Sometimes the situation in which a man finds himself may require him to shape his own fate by action. At other times it may be more advantageous for him to make use of an opportunity for contemplation and to realize assets in this way. Sometimes man may be required simply to accept fate, to bear his cross. Every situation is distinguished by its uniqueness, and there may be only one right answer to the problem posed by the situation at hand.[64]
How does one go about finding this meaning? According to Viktor Frankl, we can find it in three different ways:[65] (1) by creating a work or doing a deed; (2) by experiencing something or encountering someone; and (3) by the attitude we take toward unavoidable suffering.” In other words, meaning in life can be found not only in the external world of achievement but also in the internal world of experience, such as faith, hope, love and freedom. If suffering is avoidable, the meaningful thing to do is to remove its cause. However, if suffering is unavoidable, we may have to change our attitude toward the suffering.
One of the ways Viktor Frankl found the strength to fight to stay alive was to think of his wife and constantly keep her image before him:
My mind clung to my wife’s image, imagining it with an uncanny acuteness. I heard her answering me, saw her smile, her frank and encouraging look. Real or not, her look was then more luminous than the sun which was beginning to rise…for the first time in my life I saw the truth…the truth that love is the ultimate and the highest goal to which man can aspire…Love finds its deepest meaning in a person’s spiritual being…Had I known then that my wife was dead, I think that I would still have given myself, undisturbed by that knowledge, to the contemplation of her image.[66]
Viktor Frankl found his meaning of life and his reason for living in hope, resting in love, “the highest goal to which man can aspire.” This “love is as strong as death” (Song of Songs 8:6). Even in the degradation and abject misery of a concentration camp, Viktor Frankl was able to exercise the most important freedom of all – the freedom to determine his own attitude and spiritual well-being. No sadistic Nazi SS guard was able to take that away from him or control his soul.
To Viktor Frankl, this meaning of life, or its perception as reason for living, is completely down to earth rather than philosophical. He sees it boiling down to “becoming aware of a possibility against the background of reality…aware of what can be done about a given situation.”[67]
“It did not really matter what we expected from life, but rather what life expected from us. We needed to stop asking about the meaning of life, and instead to think of ourselves as those who were being questioned by life – daily and hourly. Our answer must consist, not in talk and meditation, but in right action and in right conduct. Life ultimately means taking the responsibility to find the right answer to its problems and to fulfill the tasks which it constantly sets for each individual.” [68]
Critique and Discussion
Friedrich Nietzsche’s proposition of free choice in arriving at personal meaning presents two problems. First, if I know that my life is based on an ungrounded, arbitrary choice, then when the going gets tough, I have no basis at all for resisting the thought that I should now simply undo what I have chosen and make a new choice. I act out a role for a time, and then, wherever my mood takes me, I move on to a different role. The result is that, though the roles all have meaning, my life has none. Life becomes absurd. This is my first reservation about freedom of choice. I believe that freedom should be well grounded in commitment. For example, in Mr. Zhang’s story,[69] Ai Yi was his reason for living. He chose to marry her against the wishes of his children from an earlier marriage. This showed commitment and love, providing good grounding for his choice. Second, if I can choose any life that I have scripted for myself, couldn’t I just as easily script myself the life of a mafia godfather as “hero,” who may be kind to animals and small children but would not stop at killing anybody in establishing my territory? Now this is just a dramatic way to make my point that freedom should also be bridled by moral responsibility.[70] When Ms. Zeng talked about choosing Physician Assisted Suicide,[71] perhaps she should also consider the moral responsibility involving not just herself but also her husband and her daughters.
Martin Heidegger appears to have solved these two problems mentioned above. By positing that the content of a meaningful life is discovered in conjunction with heritage and individual contemporary considerations rather than arbitrarily chosen, commitment is again possible. The problem of immoral script also seems to disappear, since the heritage of a culture is its morality. And yet, if I emigrate to a radically different culture, say a Chinese like myself living now in North America for over three decades, might this change not re-introduce the arbitrariness of choice, as I struggle between the two cultures, each having a different moral value?
In his later writings, Martin Heidegger proposes that there is such a thing as the universal meaning of life – the task of being the “guardians” of our world, of living in such a way that the changes we make to it are always “bringing forth” rather than violations. [72] This “bringing forth” reflects our will to conserve the fundamental order of things that is granted to us. There is a sense of awe and sacredness about the world that makes it unnecessary for us to choose whether or not we should become its guardian. This “essence” is given to us along with our existence, and not chosen by ourselves groundlessly after existence. Otto von Bismarck (of all people) advises one never to trust a man who is immune to the wonders of nature.[73] Martin Heidegger and the Taoist would agree with him. It seems that nature now represents one of the few avenues to the experience of awe that still remains open to humankind.
Even though Martin Heidegger denies many times that Being has anything to do with the God of traditional Christian theology, there is no question that Being is clearly, for Martin Heidegger, an object of reverence and awe, the object of religious feeling. In his final address to the public at large,[74] he used the title, “Only a God can save us.” Although Martin Heidegger affirms a meaning of life that is universal and discovered, this meaning is not a grand-narrative meaning. There is no associated “end of history” nor crossing a rainbow bridge into a final paradise. Rather, the task of guardianship is an ongoing and endless process. It reminds us that life is a gift that is granted to us; we should respond with gratitude and awe.
Albert Camus denies the importance of meaning in life. He says that life “will be lived all the better if it has no meaning.”[75] However, I have noticed that even in Albert Camus’ examples of absurd heroes or heroines, there is still a goal. With his hero Sisyphus, just continuing to toil without purpose, continuing to live in a world that provides no reason for living, is by itself a reason for living, if revolt is deemed his personal meaning of life. Similarly, Don Juan has his goal to seduce as many women as possible. Thus, when Albert Camus excludes “meaning” from the worthwhile life, what he means to exclude, it seems to me, is not goals as such, but rather goals of a specific nature, such as scripting one’s life in order to “build it up.” However, even with that understanding, “building” a life toward a future goal does not have to kill the joys of the present. One can still be a successful business person managing a beauty salon and be able to watch in awe the flowers bloom after the seeds are planted. [76] I think that, with an increasing awareness and practice of self-care, the present and the future can both bring joy and satisfaction.
Implications for the Terminally Ill
In all of the interviews I carried out in China, hope resting in meaning stands out as the reason for living for many of these interviewees. There was meaning found in the love and support from others. This love and support often come from family, but also from friends, from the community, as well as health care providers (physicians, nurses, etc.) and counselors (psychological and spiritual). There was also meaning found in one’s faith and spirituality, empowering the sick to live through their pain and suffering. I heard from one husband, “My wife’s new-found faith in Jesus Christ and the assurance of eternal life gave her hope to carry on.” [77] I heard from one son, “My father and I both know that God will take good care of us no matter how tough our circumstances are. We believe that all things will work for the good of those who love the Lord…miracles can happen. They will never happen without faith.” [78] I heard from one daughter, “My Lord and my God has strengthened me and walked with me…when all else fail, faith and hope sustain me and my mother.” [79] I heard from one father,“God has helped my daughter to recover from cancer. I am sure God will help me too.” [80] I heard from a dying teenager, “With Jesus by my side, my burden is light…prayer gives me the power to live another day.” [81] And the same thing went on and on. Who says God is dead? Faith provides meaning in life and in suffering, no matter how tough life may seem.
Martin Heidegger talks about being “condemned to eternal life,” a life he considers as having no meaning. He thinks that if “current life cannot tell him who he is, then an eternal life will have no meaning.” [82] Martin Heidegger sees eternal life as a future life, but eternal life is not just a life after death. It is a “godly life,” a life in which the Spirit of God is ever present with the believer, beginning from the profession of faith. Hope, which looks to the future, does give meaning to the present. As achievements are recognized, self-worth is affirmed, and confidence is assured of realizing one’s goals.
Friedrich Nietzsche talks about “personal meaning” and “personal providence” that echoes divine providence, giving assurance that everything will turn out for the best. How can one achieve this state of mind? Friedrich Nietzsche refers to it as the “psychology of the artist.” [83] In modern psychological terms, this is perception of the half-full versus half-empty glass. In reviewing the life stories of the sick, I have been encouraged by Friedrich Nietzsche’s narrative approach. Bringing out the meaning in one’s life actually helps to diminish the pain and suffering of the present, and generates enough energy in the process to sustain living through their illnesses.
It is clear that life is worth living when it is meaningful. An elderly man found his meaning and purpose in God, helping him to rekindle his will to live.[84] A dying mother’s spirit got lifted when she saw new life in the garden she had been cultivating.[85] Death takes on a new meaning when it is seen as part of the life cycle. In addition, to live in oneness with nature implies that death is good when it is a natural death. [86] Suffering also takes on a new meaning when one realizes that illness and death befall all people, just as rain falls on both the good and the bad.[87]
Furthermore, bringing up any unfinished business will also help to motivate the dying in its completion. There is hope in anticipating the realization of a goal. “My wife’s desire of seeing the birth of our first granddaughter kept her actively engaged in whatever time that still remained.” [88] “He was eager to make contact with his long lost brother to find out if his brother has any male progeny to continue the family name.” [89] “I have thought of suicide, but I can’t do it, not while my son is still getting drug rehabilitation.” [90] “I want to stay alive for the sake of my children. I hate to see them living in this cold and merciless society without a father.” [91] These were just some of the responses indicating thoughts and actions in fulfilling a purpose in life. In all of these responses, the meaning of life is very personal, chosen by each individual according to individual needs and circumstances.
Culture and heritage also provide meaning to be discovered. “My grandpa came to believe that killing himself would bring shame to the whole family.”[92] “He was disappointed in not having a grandson to pass on the family name.”[93] Here, the meaning associated with culture and heritage may or may not be adopted by the individual, who can still choose her/his own meaning.
In making health decisions, Jean-Paul Sartre claims that “we have inalienable right to choose…for ourselves.” Authenticity will give us the only meaning in life, Jean-Paul Sartre says. He encourages us to be authentic to our own true self without being bound by heritage, culture or our past. He maintains that we carry too often a lot of baggage dumped on us by culture or heritage, or by our own emotional reactions to events in the past, all of which would be best discarded if we are to live a free, fruitful, and meaningful life. His approach to life certainly has many followers, especially among the young people in China.
Friedrich Nietzsche’s alleged proposal of will to power as a personal meaning of life has drawn considerable criticism. Whether he meant power over others or power over oneself remains unclear. However, another way of interpreting this is to consider this will to power as a will to retain control over one’s life. This is particularly important for patients who have lost much of their personal control. They are to take off their clothes in the cold examination rooms without a whimper, to stay awake in their hospital beds for the doctors to come and make rounds, and left with little dignity when tubes go through every body orifice. The will to retain control or power in those instances makes a lot of sense.
Georg Hegel’s promise of a good ending down the line (history or time-wise) can be very comforting. His concern about human alienation also speaks well to the terminally ill who tend to retreat into their own corners to avoid embarrassment or hurt. His assurance of a future world filled with peace and harmony reminds us of the “city of God” in the Christian tradition, even though Georg Hegel is an atheist. Georg Hegel’s belief in “utility” as a criterion of existence is the beginning of utilitarianism in ethical consideration of one’s “duty to die.” His notion of “nothing exists unless it has utility” also has obvious socio-political implications in the consideration of euthanasia, especially in the terminally ill, when the general will clashes with the individual will.
In the time I spent with the terminally ill and their caregivers (both family and professional) in China, I heard from them the same questions over and over again: “Why does this happen? I am still young. I am not supposed to have cancer. If there is a God who is love, why this torment?” [94] “She never smokes – why lung cancer?” [95] I have no good answer to these questions. The analogy invoked by Viktor Frankl makes a lot of sense.
“Consider a movie. It consists of thousands upon thousands of individual pictures, and each of them makes sense and carries a meaning, yet the meaning of the whole film cannot be seen before its last sequence is shown. We simply cannot understand the whole movie without having first understood each of its components, each of the individual pictures. Isn’t it the same with life (and suffering)? Doesn’t the final meaning of life (and suffering), too, reveal itself, if at all, only at its end, on the verge of death? And doesn’t this final meaning, too, depend on whether or not the potential meaning of each single situation has been actualized to the best of the respective individual’s knowledge and belief?” [96]
When I
hear the cliché, “It is not how long we live, but how we live that is important,”
the words of Rachel Naomi Remen, one of the earliest pioneers of mind/body
health, come to mind, “Health is not a goal; it is a means to doing what is
purposeful or meaningful in life.” [97] In
the next chapter, we will discuss this hope that “orients us to a flourishing
whole,” a hope that “empowers us” to find a purposeful and meaningful life, and
a hope that “sustains us” in our tribulations. [98]
[1] Interview #8, Appendix.
[2] Refer to her story in Chapter 2, page 53-55 in dissertation. Interview #12, Appendix.
[3] A narrative is a story: an interpretation of some aspect of the world that is historically and culturally grounded and shaped by human personality.
[4] David Wong, “Comparative Philosophy.”
[5] Plato, Plato’s Phaedrus, trans. Reginald M. Hackforth (London: Cambridge University Press 1952), 247d.
[6]Ibid., 247b.
[7] Plato, The Republic, introd. Charles M. Bakewell (New York: Charles Scribner, 1928),Book 7, 518C, 278.
[8] Aristotle, Nicomachean Ethics, trans. Roger Crisp (Cambridge: Cambridge University Press, 2000), Book II.6-7, 34.
[9] Julian Young, The Death of God and the Meaning of Life (London: Routledge, 2003).
[10] Immanuel Kant, Critique of Pure Reason, trans. John Miller Dow Meiklejohn (Mineola, NY:Courier Dover Publications, 2003), 238.
[11] Kant, 41-42.
[12] Ibid., 377.
[13] Arthur Schopenhauer, The World as Will and Representation, vol. 2, trans. E. F. J. Payne (Indian Hills, CO: Falcon’s Wing Press, 1958), 182.
[14] In the words of Friedrich Nietzsche, The Will to Power, trans. Walter Kaufmann and R. J. Hollingdale (New York: Vintage Press, 1968), sect. 1005.
[15] Friedrich Nietzsche, The Gay Science, trans. Walter Kaufmann (New York: Vintage Books, 1974), 109.
[16] Schopenhauer, World as Will and Representation, 324.
[17] Friedrich Nietzsche, The Birth of Tragedy and the Genealogy of Morals, trans. Francis Golffing (New York: Doubleday 1956), 124.
[18] Friedrich Nietzsche, The Birth of Tragedy, trans. Walter Kaufmann (New York: Vintage Press, 1966), 21.
[19] Ibid., 17.
[20] Ibid., 5.
[21] Nietzsche, Will To Power, section 1005.
[22] Nietzsche, Birth of Tragedy, 10.
[23] Georg Wilhelm Friedrich Hegel, Phenomenology of Spirit, trans. Arnold V. Miller (Oxford: Clarendon Press, 1977), Preface.
[24] Ibid., parag. 642.
[25] Nietzsche, Birth of Tragedy, 26.
[26] Hegel, Phenomenology of Spirit, paragraph 584.
[27] Ellen Ott Marshall, Though the Fig Tree Does Not Blossom: Toward a Responsible Theology of Christian Hope (Nashville: Abingdon, 2006), 98.
[28] Nietzsche, Gay Science, 125.
[29] Ironically, this term is a creation of philosophers in the United States who focus on the work of post-Enlightenment thinkers in the European continent, especially those in France and Germany. It is an umbrella concept that covers many movements, including German idealism, phenomenology, and existentialism. See “Intersections between Pragmatist and Continental Feminism,” Stanford Encyclopedia of Philosophy, http://plato.stanford.edu/entries/femapproach-prag-cont (accessed May 20, 2008).
[30] Nietzsche, Gay Science, 108.
[31] Nietzsche, Will to Power, section 2.
[32] Nietzsche, Gay Science, 4-5.
[33] Nietzsche, Gay Science, 78, 335.
[34] Marshall, 97.
[35] See Ch. 3, page 71. Interview #8, Appendix.
[36] See Ch. 2, page 54. Interview #12, Appendix.
[37] Friedrich Nietzsche, Thus Spake Zarathustra, trans. Thomas Common (New York: Heritage Press, 1967), 20.
[38] Nietzsche, Gay Science, 277. This saying resonates well with what the Christian Bible says, “All things work for the good of those who love the Lord” (Paul’s Letter to the Romans, 8:28).
[39] Reminiscence is defined as “the act or process of recalling past events or experiences” in Webster’s College Dictionary (New York: Random House, 1950).
[40] Friedrich Nietzsche, “Twilight of the Idols,” in The Portable Nietzsche, trans. and ed. Walter Kaufmann (New York: Penguin, 1976), IX, 8.
[41] Friedrich Nietzsche, The Genealogy of Morals, trans. Walter Kaufmann and R. J. Hollingdale (New York: Vintage Press, 1968), I, 10.
[42] Nietzsche, Gay Science, 370.
[43] Martin Heidegger, Being and Time, trans. John Macquarrie and Edward Robinson (Oxford: Blackwell, 1978), 384-85.
[44] Story (at beginning of Chapter 2) from Interview #6, Appendix.
[45] Albert Camus, The Myth of Sisyphus, trans. Justin O’Brien (London: Penguin, 2000), 11.
[46] Ibid., 14-19.
[47] Camus, The Myth of Sisyphus, 7.
[48] Ibid., 53.
[49] Ibid., 133.
[50] Story of Ms. Zeng in Chapter 2 of this dissertation, page 54. Interviewee #12 in Appendix.
[51] Ibid.
[52] Arthur Schopenhauer, Parerga and Paralipomena: Short Philosophical Essays, trans. E.F.J. Payne (Oxford: Clarendon Press, 1974), 2:285-86.
[53] Quality of life as defined by the Center for Disease Control and Prevention, Atlanta, Georgia, http://www.cdc.gov/healthyplaces/terminology.htm (accessed May 24, 2008).
[54] Anna Donald, “What is Quality of life?” 1st ed. (2003), http://www.whatisseries.co.uk/whatis/pdfs/ what_is_QOL.pdf (accessed May 25, 2008).
[55] Jerome R. Wernow, “Saying the Unsaid: Voicing Quality-of-Life Criteria in an Evangelical Sanctity-of-Life Principle,” Journal of the Evangelical Theological Society 391, no. 1 (March 1996): 103-22.
[56] John Dunlop, “A Physician’s Advice to Spiritual Counselors of the Dying,” Trinity Journal 14, no. 2 (Fall 1993), 206.
[57] Frankl, Man’s Search for Meaning, 12. Originally published in 1946 as Trotzdem Ja zum Leben sagen: Ein Psychologe erlebt das Konzentrationslager.
[58] Frankl, Man’s Search for Meaning, 141.
[59] Ibid., 133.
[60] Ibid., 116.
[61] Ibid., 139.
[62] Frankl, Man’s Search for Meaning, 136.
[63] Ibid., 82.
[64] Ibid., 85-6.
[65] Ibid., 115.
[66] Frankl, Man’s Search for Meaning, 49-50.
[67] Ibid., 145.
[68] Frankl, Man’s Search for Meaning, 85.
[69] Mr. Zhang’s story from Interview #8, Appendix. Also see Chapter 3.
[70] Young, Death of God, 120.
[71] Ms. Zeng’s story from Interview #12, Appendix. Also see Chapter 2.
[72] Martin Heidegger, The Question Concerning Technology and Other Essays, trans. William Lovitt (New York: Harper & Row, 1977), 28.
[73] Otto von Bismarck, cited by Charles B. Guignon, The Cambridge Companion to Heidegger, 2nd ed., rev. (Cambridge: Cambridge University Press, 2006), 390. Publication information for Bismarck not provided.
[74] 1966 interview with the German magazine Der Spiegel.
[75] Camus, Myth of Sisyphus, 53.
[76] Ms. Zeng in Interview #12, Appendix.
[77] Interview #1, Appendix.
[78] Interview #2, Appendix.
[79] Interview #3, Appendix.
[80] Interview #4, Appendix.
[81] Interview #14, Appendix.
[82] Martin Heidegger’s assertion that I am the only person fit to run my own life is, in a way, resonant with Martin Luther’s assertion that the ultimate authority which determines the right and the good is my own conscience. Thus, it can be argued that Martin Heidegger’s “authenticity” can be seen as preserving the essence of a Christian theology in spite of the pronouncement of “God is dead.”
[83] Nietzsche, “Twilight of the Idols,” IX, 8.
[84] Interview #2, Appendix.
[85] Interview #20, Appendix.
[86] Interview #21, Appendix.
[87] Interview #16, Appendix.
[88] Interview #1, Appendix.
[89] Interview #7, Appendix.
[90] Interview #15, Appendix.
[91] Interview #6, Appendix.
[92] Interview #7, Appendix.
[93] Interview #7, Appendix.
[94] Interview #12, Appendix.
[95] Interview #10, Appendix.
[96] Frankl, Man’s Search for Meaning, 145.
[97] Rachel Naomi Remen, cited in Healing and the Mind by Bill D. Moyers, Betty S. Flowers, and David Grubin (New York: Doubleday, 1993), 357. Publication information for Remen not provided.
[98] Marshall, Though the Fig Tree Does Not Blossom, 97.
CHAPTER 4: Hope
Ms. Yu, a church member, asked me after our Bible study group session what I thought of a drug called Iressin. She knew I was a doctor before. This drug was apparently prescribed for her mother Li-ying.[1] Ms. Yu was concerned about the cost and efficacy of this drug. Really, I knew very little about this drug, but I promised her that I would look it up.
I have met her mother before. It was a year ago. I went to visit her in the hospital when she was investigated for a chronic cough. That unfortunately turned out to be lung cancer with a poor prognosis. The doctors suggested chemotherapy to buy some more time, but the family did not wish to alarm the patient for fear that Li-ying would just give up hope altogether.
Ms. Yu agreed with me that I should pay her mother a visit. She gave me a ride on her motorcycle. They lived in a busy part of town. On the ground floor of their apartment building were shops that included a noodle place, a travel agency, and a stationery store. Many motorcycles were parked along the curbside. They had become a very popular means of transportation. The droves of bicycles in the 1990s had disappeared and were replaced by increasing number of motorcycles and cars on the road.
We walked up to the third floor and were greeted by Li-ying. The past year had changed her considerably. The stocky woman I knew had become a shadow of what she used to look like. She appeared to have aged by at least ten years, with a shriveled face and sunken eyes. One thing that had not changed was her engaging smile.
“Where were you this past year? What took you so long to come and visit an old lady like me?” Li-ying said.
“Old lady? Where?” I replied in jest. “I went home to America and just got back. How have you been, Li-ying?”
“This cough is killing me. I don’t understand it. It’s been a year and a half now. Still there is no improvement. The doctors don’t seem to know what’s going on.”
“Mom, didn’t the doctors want you to be admitted to the hospital for more tests? Why won’t you go?” Ms. Yu, the daughter, interjected.
“Xiao bao-bao (Little darling), it will cost a lot. I am getting old and useless. Why spend so much money on me? I’d much rather see you save this money up for your wedding. I have been waiting for you to get married and have a baby for a long time now.”
“Mom, if you are not feeling well, that money has to be spent. Besides, I just got a new job. It’s not a lot of money, but at least it puts food on the table. We can no longer eat off the land anymore, can we?”
“Yeah, Xiao bao-bao. Rice is a beautiful crop,” Li-ying said wistfully. “I still remember the harvest time. All of the rice paddies turned a beautiful bright golden color. I love the sight of the heavy clusters of grain hanging over at the top of each plant. I remember working in the ripening fields with other women, laughing and joking with one another, while hanging scarecrows, cloths, and ropes in the ripening rice fields to scare away the birds. Farming is hard work for us women. We work in the field as well as taking care of our household work. The harvest makes it all worth while. We cut the ripe rice stalks, bundled them up to be dried under the sun, and hauled them to the threshing ground. I love to return to the field and see the harvest once more, if only for the last time.” Tears came to her eyes as she said this.
“Mom, we love you. We want you to be happy,” daughter said hastily.
“Li-ying, we all love you,” I added. “It must be rough for you to feel this degree of apprehension and fear about the future, having been stricken with an illness that you don’t fully understand, and grieving over the loss of your health, your youth, your circle of friends and your self-worth in utility terms. I do admire you for who you are – your unswerving commitments to your family, your faithfulness at work, and the love and concern you show to others. Just as you marvel at the beauty of the golden harvest, your family and your friends will marvel at the love you have shown them and the beauty of your faithfulness.”
“I am very grateful for all this support from all of you. Yes, it is a wonderful life. I hope to keep it that way. Thank you so much for your visit.”
It was on that note of hope that we parted company. Even though death was imminent, Li-ying could appreciate the beauty of a simple and natural life and taste the sweetness of its fruit. The Taoist is right. Nature can be so awesome as to take our breath away. Just as Martin Heidegger declares, nature seems to now represent one of the few avenues to the experience of awe that still remains open to humankind. Cherishing the thought of returning home to the wonderful life in the farm and the hope of seeing her daughter get married, Li-ying persevered in her tribulations. She died four months later.
What is Hope?
Hope is a word used often, yet the definition is not conclusive. In the Merriam-Webster Dictionary, the verb “hope” means “to cherish a desire with anticipation; or expect with confidence.” It involves desiring and patiently expecting with confidence something or someone to provide a certain good in the future. In the Scripture of Judeo-Christian faith, the noun “hope” denotes trust in God, the object of hope. [2] To Thomas Aquinas, hope is a virtue that takes as its object “a future good, difficult but possible to obtain.” [3] In psychological terms, Charles Snyder defines hope as the sum of the mental will-power and “way”-power that a person has for achieving goals. [4] To Andrew Lester, hope is a configuration of cognitive and affective responses to life that believes the future is filled with possibilities and offers a blessing. [5] Erik Erikson defines hope as an attitude, “the enduring belief in the attainability of fervent wishes.” [6] From this assortment of definitions, one can see that there are some difficulties in defining hope.
Hope seems to be one of those features of human life that we think we know and understand until we try to say something about it. The more we try to say what we think it is, the more it seems to defy our best efforts to do so. Donald Capps points out that some of the confusion in talking about hope is perhaps due to the failure to make a distinction between “hoping” and “hope.” [7] “Hoping” indicates that we are dealing with aprocess or form of experience, one that may be compared with other experiences, like “loving,” “creating,” and the like. The noun “hope,” on the other hand, concerns a phenomenon or thing, one that may be compared with other things, like “belief,” “judgment,” or “skill.” Thus, Donald Capps would define “hope” as the perception that what one wants to happen will happen, a perception that is fueled by a persistent desire in response to felt deprivation. He further defines “hope” as a projection that envisions the realizable goal. From a pastoral perspective, Ray Anderson defines hope as the vision which is seen with the eyes of faith and which satisfies the deepest longing of the heart. [8]
In addition, when defining hope, it is just as important to point out what hope is not. [9] First, hope is not optimism. Hope does not pertain to easy or certain things, no matter how good they may seem and how much we miss them right now. Hope is tough. Hope knows there are difficulties and realizes what it will cost to deal with them. Second, hope is not acquiescence. Precisely because hope deals with difficulties, it requires hard work. The process of pursuing the object of hope is arduous. Hope demands active engagement, and in fact, hope enables action in difficult times. We do not embark upon a difficult course of action unless we have the hope that we will succeed. Third, hope is usually not solitary. The fulfillment of hope frequently requires acts of love or support from others. This support can come from family, community, friends, health care providers (such as physicians and nurses) and counselors (both psychological and spiritual).
The Earliest Virtue
Ideally, we live our lives from the implicit conviction or tacit belief that the future is open-ended with possibilities. We do not necessarily believe that everything will go well, nor are we necessarily optimistic about what the future holds for us, but we are hopeful and act from hope.
Two psychologists, Erik H. Erikson and Paul W. Pruyser, both in the psychoanalytictradition, argue that this attitude of hope can be traced to our earliest experiences of life as infants. Erik Erikson’s major statement on hope appears in his article, “Human Strength and the Cycle of Generations.” [10] He notes that during an individual’s life cycle, there are certain strengths that he named as “virtues.” In Old English, virtue meant “inherent strength” or “active quality,” and referred to the undiminished potency of well-preserved medicines and liquors. Thus, “virtue” and “spirit” once had interchangeable meanings. By calling these human strengths “virtues,” Erik Erikson proposes that there are eight such virtues, each being closely linked to the psychodynamics of a given stage of an individual’s life cycle. These virtues include hope as the earliest virtue in development, followed by will, purpose, competence, fidelity, love, care, and wisdom.
To the extent that strengths build upon prior strengths, this means that hope is the basis for all other strengths. Erik Erikson does not claim that hope is the most important in some normative sense, because, after all, he is well aware that the Apostle Paul in the Christian tradition considered love to be greater than either hope or faith. Yet, for Erik Erikson, developmentally speaking, hope is the most important one, because every other virtue builds on it: “Hope is both the earliest and the most indispensable virtue inherent in the state of being alive.” [11] If a hopeful orientation to life fails to develop, all subsequent strengths – including love – are thereby diminished.
Erik Erikson defines hope as “the enduring belief in the attainability of fervent wishes.” [12] His view that hope is an “enduring belief” suggests that it is not a strength that suddenly disappears as we move beyond the life stage in which this strength emerged, but, rather, it continues to influence our development throughout life. Furthermore, his suggestion that hope endures indicates that hope is threatened by other perceptions and emotions (like despair, apathy, and guilt) [13] with which it coexists. Yet Erik Erikson believes that it is better that way: “An exclusive condition of hopefulness, translated into various imaginable worlds, would be a paradise in nature, a Utopia in social reality, and a heaven in the beyond. However, in the individual, here and now, it would mean a maladaptive optimism.” [14] In Erik Erikson’s view, it is this endurance that separates hope from optimism.
What inspired Erik Erikson to locate hope in the earliest stage of life? Erik Erikson first noted that others have called this earliest positive attitude “confidence,” and that he himself had called it “trust.” But he asked, “What is it that sustains life even where confidence is wounded and trust impaired?” The answer, he says, is hope. [15] Hope is a basic strength precisely because it persists even when we have no objective grounds for trust. Throughout life, hope, as a basic human quality, exists independently of the realization of specific hopes: “Hope, once established as a basic quality of experience, remains independent of the verifiability of ‘hopes,’ for it is in the nature of our maturation that concrete hopes will, at a time when a hoped-for event or state comes to pass, prove to have been quietly superseded by a more advanced set of hopes.” [16] Thus, hope becomes an attitude toward life and, as an attitude, it does not depend solely or even primarily on the attainment of specific hopes.
Another basis for viewing hope as the quality that emerges in the earliest stage of life is the fact that “there is something in the anatomy even of mature hope which suggests that it is the most childlike of all ego-qualities.” [17] One can observe such childlikeness in the supplicatory prayers of adults as they assume a measure of childlikeness toward unseen, omnipotent powers.
Hope is essential to the interactions that occur between infant and caretaker (often the mother) with whom the infant interacts: “The infant’s smile inspires hope (in the mother) and, in making her smile, makes her wish to give hope (back to the infant).” [18] This reciprocal experience is very important. It is through this trusting relationship that hope originates in the infant. The critical factor in infancy is the secure apperception of a first love-object; that is, experiencing the mothering person as a coherent and trustworthy being, who reciprocates our physical and emotional needs in expectable ways. These objects, which can be things or persons, are for the infant “the first knowledge, the first verification, and thus the basis, of hope.” [19]
Erik Erikson places particular emphasis on the mothering person as verifier of hope, which applies not only to the world of persons, but also to the world of things. “To the human infant, mother is nature.” She represents not only “coherent being” but also “thing world” for the infant. Through her, the infant discerns the enduring quality of things as well as of beings. Thus, Erik Erikson stresses the unique role of the mothering person as the basis of hope: “She must be that original verification, which, later, will come from other and wider segments of reality.” [20] This mothering person provides “a convincing pattern of providence” [21] in which hopes are met and hopefulness becomes inherently rewarding. Our perception of ourselves, our self-identity, or a sense of I-ness, is also rooted in the same experiences that engender and verify hope. [22] In these experiences, the infant acquires a sense not only of the enduring quality of things and other beings, but also of his or her own enduring nature.
Clifford Scott has suggested that hoping is part of a dynamic sequence of wishing to waiting, to anticipation, to pining, and then to hoping, [23] but Paul Pruyser believes that hoping is oriented to reality, whereas wishing is not. In an infant-mother relationship, the infant discerns that the “benevolently disposed object” [24] (the mother) desires to satisfy her/his longing, whereas the mother also discerns that the infant desires to satisfy her own longing. When each discerns that the meeting of the desires of one person will fulfill the desires of the other, hope arises, with a kind of intuitive knowing or subjective certainty. Based on this subjective certainty that one’s desires will be reciprocated, Paul Pruyser suggests that hoping is reality-oriented and different from wishing. [25]
Hope can arise when the one-caring and the cared-for meet each other’s needs. The sixteen-year-old granddaughter who looked after her debilitated grandpa was hoping that he would treat her better as a person, even though she was not a boy as he had hoped for. [26] That was her need, the need of recognition and acceptance. It must have been a touching moment when he finally thanked her for her filial piety and unwavering commitment to his care. By recognizing these qualities in her, he was meeting her need; and his own need was met too, when he recognized that his desire of having a loving and faithful grandchild had been largely met. As each person verifies hope in the other, hope is being fostered. This hoping applies not only to the world of persons, but also to the world of things as well. [27] Love and support will go a long way in fostering hope. Paul Pruyser is right in what he says about hoping: “in hoping…(there is a) positive balance of love, which can encompass, restitute, and repair effects of hate.” [28]
Development of Hope
As the infant grows into a child, hope inspires acts of will, which is the second virtue after hope. While the earliest experience of hope in infancy may involve an initiative such as a smile or an outstretched hand from the infant, this initiative will increase as the infant becomes a child. Hoped-for events are not just longed for but are sought after. There will also come about a greater capacity to renounce one’s hope, to “transfer disappointed hopes to better prospects,” and to train our expectations “on what promises to prove possible.” [29] Hope becomes increasingly identified with change, new prospects, and widening horizons. In this new milieu, hope becomes more flexible and adaptable. We may no longer insist on having the precise object of our desire, but may accept substitutes of comparable worth. We may become more discriminating in what we hope for as we discern a closer fit between what we desire and what is possible. And most important of all, we remain hopeful even when we do not attain what we hope for. In this second stage of the life cycle, persistent hopefulness becomes an attitude (or strength) that arises partly from our increased capacity for renunciation of our desires but primarily from the projective character of hope. Even as certain hoped-for events are coming to pass, they have already been “quietly superseded by a more advanced set of hopes.” [30] Thus, our hopefulness does not depend on the realization of any particular hope. This hopefulness has become intrinsic to who we are, and will continue to develop throughout our life cycle.
Chinese Perspectives on Hope
The word “hope” can be expressed in different Chinese connotations: hope希望 also means desire盼望/期望 (wish 願望), or faith (trust信心; reliance信赖) or a sense of anticipation (future expectation期待). In addition, hope also connotes endurance (patience忍耐; perseverance 堅定). All of these characteristics can be demonstrated in the stories I heard in my field work. The people I interviewed used the word “hope” quite freely without prompting. It seems to give them a glimpse of the future that would bring them present peace and contentment. One father who had accepted the terminal nature of his illness did find peace in the hope that his son would soon get full rehabilitation from drug addiction. [31] Another mother would not give up in her fight against cancer until she was content that her daughter had given birth without complication. [32] In their suffering, the Chinese people are learning to accept and endure, to embrace life in its totality (promises and perils), and to integrate both their positive and negative life experiences. Acceptance does not have to exclude hope.
Contentment is a big part of the Chinese psyche. It involves overcoming cravings when times are good and overcoming worries when times are bad. Thus, contentment is always there regardless of reversals of fortune. Contentment also comes with a humble, selfless devotion to the well-being of humanity. One Christian woman found fulfillment in life when praying for others in need while her cancer was slowly sapping her strength away. [33]
Many Chinese hope to live a plain life in peace and harmony with one’s family and neighbors. Happiness is found in harmonious relationships. One Chinese idiom says, “Everything will be alright, when there is harmony at home.” No wonder one father in hospital pulled out his intravenous drip when he saw his children squabbling over the management of his debilitating stroke. [34] His hope of seeing harmony at home was squashed, and he felt he no longer had any reason for living.
For the Confucians, utopia 大同 is their object of hope, when there will be universal order and harmony. The utility of efforts by each individual will contribute to the common good.
“When the perfect order prevails, the world is like a home shared by all. Virtuous and worthy men are elected to public office…peace and trust among all men are the maxims of living. All men love and respect their own parents and children, as well as the parents and children of others. There is caring for the old…there are nourishment and education for the children. There is a means of support…for all who find themselves alone in the world; and for the disabled. Every man and woman has an appropriate role to play in the family and society. A sense of sharing displaces the effects of selfishness and materialism. A devotion to public duty leaves no room for idleness…The door to every home need never be locked and bolted by day or night. These are the characteristics of an ideal world, the commonwealth state.” [35]
The state can offer the means of achieving this goal, and individuals will remain conscientious, work hard and persevere to reap their benefits. At this moment, the State Council of China is working feverishly on health care reforms to make health care more accessible and more affordable to every one of her citizens.
In another sense, Confucius’ teachings on virtues like filial piety, loyalty and respect, especially in the context of family relationship and friendship, have lent a great deal of support to the care of the terminally ill. We have seen time after time loving and loyal family members and friends committing unwaveringly to the aid of these people in despair and cheering them up, fostering in them not just a meaning of life, but a reason for living. However, filial piety can have its negative side too. Chinese tradition has it that the children have a duty to keep their parents’ best interest in mind. This includes keeping the parents happy and contented, safe and healthy throughout their lives. It is inevitable that the children would opt for more aggressive treatment for their parents out of a sense of filial duty.If they do not, others in the community would point a finger at them, criticizing them for not looking out for their parents’ best interests. [36]
Furthermore, the Confucian notion of legacy ties in the present generation to the past and to the future. The hope of honoring one’s ancestors and passing on a worthy legacy to the next generation helps the terminally ill to transcend their pain and suffering. In the Chinese mindset, suicide out of despair brings dishonor to one’s family name. On the other hand, a worthy legacy to be passed on to the next generation may be spiritual (as in eternal life), biological (as in blood lineage), relational (as in harmonious family relationship), experiential (as in meaning), moral (as in virtues), cultural (as in family name), and financial (as in inheritance).
What about hope in Buddhism? Even though a Buddhist sees life as bitter and suffering as part of life, Buddhism offers joy and hope to those who suffer. The experience of suffering is the greatest challenge to hope, and yet it is also true that suffering produces hope. The hope of attaining enlightenment and eternal bliss (nirvana) is in every believer, and a path of achieving that realizable good is provided. Geoffrey DeGraff describes with clarity how suffering should be viewed through the lens of hope. [37] He describes the process of hope as a series of small steps. It is as if one is climbing a ladder to get onto the rooftop. You start with the first rung of the ladder, mindfulness; then you grab hold of a higher rung so that you can let go of the lower one, and then grab onto a rung still higher. As the rungs get further off the ground, your view gets more expansive, and you can concentrate on precisely where the mind’s cravings are. In other words, you get a sharper sense of which part of that experience belong to which Noble Truth and what should be done with them: the parts that are suffering should be comprehended (accepted); the parts that cause suffering should be abandoned (by taking action to rid the causes); the parts that form the path to the end of suffering should be further developed (allowed to grow spiritually); and the parts that belong to the end of suffering should be verified. This will help you to get higher and higher on the ladder until you find yourself securely on the roof. That’s when you can let go of the ladder and be totally free. Suffering causes you to climb that ladder. In a way, suffering is also your teacher, Geoffrey DeGraff claims. Through this experience, you reach that transcendental state of serenity and enlightenment that Buddhists call nirvana, or eternal bliss, the goal of every Buddhist. Suffering will have come to an end, and hope is thereby verified.
Geoffrey DeGraff suggests that anyone who thinks of death as an end to suffering has misunderstood the First Noble Truth. Who would know what the next life is like? It could be worse than this one. Instead, Geoffrey DeGraff proposes that we can negotiate life, armed with all four Noble Truths, realizing that life contains both suffering and an end to suffering. Then there will be hope, a hope that someday, in this life, suffering will come to an end.
The Taoist belief in the duality of nature has influenced many Chinese too, prompting them to embrace and integrate both the light and the dark sides of life circumstances and grow from that practice of hope, taking into consideration both the perils and the promises. The good does not exist without the bad. Bliss does not exist without suffering. Lao-zi observes: “Fortune owes its existence to misfortune, and misfortune is hidden in fortune.” [38] Therefore, we should not be depressed when times are bad or overjoyed when times are good. Life is sour and bitter, but it is also sweet. Despite fear, there is hope. They are both perceptions of the mind, and if we are in touch with our true self (the Tao), then there is no need to fear, and there is everything to hope for. Since everything in nature is cyclical, there is always the hope of ending the suffering. “Hope and fear are both phantoms that arise from thinking of the self. When we don’t see the self as self, what do we have to fear?” [39]
As a result of their history and the limited resources available to them, the Chinese people often cling to hope in dealing with the vicissitudes of life. They learn to change themselves in order to cope with uncontrollable circumstances and an unpredictable future. They respond to these changes with acceptance, tolerance, flexibility, and accommodation. They strive to anticipate difficulties and patiently engage them with endurance and confidence. Their open-mindedness and intuition enable them to explore possibilities and alternatives. They envisage a better world ahead through faith. They work diligently to reach out to the future and achieve their anticipated goals. They collaborate with each other in trust and harmony, and remain humble in the service of others. And yet, despite many of these virtues and strengths, they have their weakness and vulnerability. There are times when the enemies of hope hit them like a train, injecting them with apathy, despair and shame. These are times when they feel that life is no longer worth living, times that make them wish for “good death” rather than “good life.”
Western Perspectives on Hope
Dimensions of Hope
Carol Farran, Kaye Herth and Judith Popovich have proposed a four-dimensional model of hope. This will help us to compare hope with meaning that makes life worthwhile. These three nursing educators and researchers describe hope as having four central dimensions or attributes: an experiential process, a relational process, a spiritual or transcendent process, and a rational thought process. [40]
Hope as an Experiential Process. If we attempt to understand hope, we are soon confronted with the dialectical relation between hope and hopelessness. That is, to learn more about hope, we must also learn more about hopelessness, and vice versa. Thus, even when hope has been studied extensively as a concept in the literature, hope has to be experienced in the face of some inescapable “trial” or suffering such as cancer or Acquired Immune Deficiency Syndrome (AIDS). This suffering is more than just a stressful life event. It includes a sense of powerlessness, or a potential hopelessness associated with the inability to change one’s external circumstances. Despite such inability, “any man can, even under such circumstances, decide what shall become of him – mentally and spiritually.” [41] Hope resting in a personal meaning of life can still be found in one’s internal world of experience. In our story, even though Li-ying could not prevent her body from wasting away, or stop grieving over the loss of her youth, her health, her friends and her usefulness, she could still hope for her day in the sun at harvest time, and for the joy of seeing her daughter get married. [42] She had found meaning in her life, bringing the harvest home and enjoying the fruit of bringing up her daughter. This meaning in her life gave her zest for living and hope for better days. We do not know the exact sequence of events that enabled Li-ying to hope despite adversity, but we can only speculate that perhaps her experiences with seeing the rice stalks ripen, the beauty of the golden harvest, and the fruit of her labor (both in the field and at home) might have provided the foundation of her hope, because they were meaningful to her. Her willingness to “bring out the major achievements of her life” had swept away “the petty and the inconsequential.” [43] Friedrich Nietzsche makes a valid point here.
Hope as a Relational Process. Hope thrives on intimacy and rests in love and support. Family, friends, and caregivers contribute to the maintenance of hope. Gabriel Marcel was one of the first to relate the phenomenon of hope to love. Jean Nowotny, who translated for Gabriel Marcel, described Gabriel Marcel’s position this way:
“The phenomenology of hope reveals an unconditional element at the heart of hope, a demand that love should have an absolute foundation. Since hope seeks its fulfillment in love, then hope also requires faith in an absolute Thou who secures and confirms the communion of love. In hope, love and faith are united.” [44]
Hope for Gabriel Marcel “involves a mutual trust between persons and is ultimately a response to a Thou.” [45] This resonates with Erik Erikson’s description of the origin and development of the hopeful self in the trusting atmosphere of infant-mother relationship. Unconditional love from the mother can verify hope in the infant, just like the “absolute Thou” who is “the transcendent source and guarantee of absolute hope.” [46] In the ideal infant-mother relationship, each discerns that the meeting of the desires of the other will fulfill the desires of the self.
Mainstream Christian theology has always believed that human beings are created in God’s image, so it is expected that human beings will reflect part of that divine personhood. Since by nature the triune God is a communal being, with interaction between God the Father, God the Son, and God the Spirit, human beings are relational too. The Christian community also believes that God’s nature is characterized by the unconditional and self-sacrificing love called agape. Since love, by its nature, must express itself in relationship, then God must be a relational God in this sense too. So are human beings.
For Gabriel Marcel, love and hope are close allies. Love does not make sense unless there is a relationship in which this love can be expressed and lived out. For this reason, Gabriel Marcel says, “Hope is only possible on the level of ‘us,’ or we might say, of the agape, and that it (hope) does not exist on the level of the solitary ego.” [47] Schubert Ogden says the love of God “is itself the object of Christian hope as well as its ground.”[48] Since hope is grounded in God’s love, and love implies relationship, then hope must happen in community, whether between human beings or between human beings and God.
Hope as a Spiritual Process. Like the other genuine feelings (for instance, sorrow and joy), hope is not possible without spirit, because it arises only out of, or in spiritual connection with, and through, the spirit. The Jewish theologian, Abraham Heschel, suggests that, while our passions move us, it is spirit which gives the direction and goal to the self and which empowers hope. “While spirit includes passion or emotion, it must not be reduced to either. Spirit implies the sense of sharing a supreme super individual power, will or wisdom. In emotion, we are conscious of its being our emotions, whereas in the state of being filled with spirit, we are conscious of joining, sharing or receiving “Spirit” from above (Isaiah 32:15). Passion is a movement; spirit is a goal.” [49] “The source of hope is thus the “filling of Spirit” which empowers the self to release the longing of faith toward the goal which hope sets forth.” [50]Christianity affirms that there is a created human spirit which is given by God through the mystery and miracle of birth. It also affirms the reality of the Spirit of God, which is communicated to the self and moves within each believer, so that they can experience in their hearts the power of hope in their lives.
Philosophers and theologians alike maintain that hope is inseparable from faith. For many, hope and faith are based on a spiritual structure. Faith cannot be sustained without hope. Hope is a “steadfast anchor of the soul” (Heb. 6:19). The spiritual power of hope produces the capacity in people to embrace loss and suffer disability without losing faith in life. Similarly, hope has no basis without faith. [51] Hope has been characterized as faith in oneself and others, a conviction about something that has not yet been proven, or a sense of certainty about that which is uncertain.
The ability to transcend difficult circumstances is often associated with the spiritual or transcendent attribute of hope. Hope can have spiritual power to take up and carry the burdens of life. Even when suffering from constant pain, one Christian lady I met in her death bed was still able to express the spiritual attribute of hope through an active prayer life.
Hope as a Rational Thought Process. It is in the second or early childhood stage of development that hopefulness itself assumes a new dimension, a process of thought and action. Hope becomes less associated with awaiting the mothering person and more related to the child’s emerging capacity to take independent actions, some of which may be contrary to the desires of the mothering person. As the infant becomes a child, with increasing desires and capacity to make choices, a sense of personal autonomy emerges, with which hope is closely associated. The desire behind the child’s hope is not only for the expected appearance of the mothering person, but also for the freedom to think and act while exercising personal choice.
This fourth dimension of hope is the most common dimension in psychological research. It has five components: goals, resources, steps taken, control, and time consciousness.[52] To be rational, the desired goals must be realizable, and have enough resources to support them. Active steps, even small ones, must be taken toward attaining these goals. A certain sense of control is essential; without it, feelings of powerlessness or hopelessness would set in. Finally, there should be a sense of past, present, and future, since hope looks to the future. All these components point to a rational thought process in hope. When Ms. Zeng talked about her hopes, she was not just optimistic or wishful.
“I hope to live life to the fullest. Life is filled with such wonderment and awe. I hope to spend more time with my husband and with my children, holding each other in sweet embrace. I hope to work creatively as a hair stylist as long as I am able to. I hope to continue gardening and watch in awe the flowers bloom after I plant the seeds. They say cats have nine lives. I only have one. Might as well enjoy the time I have now.” [53]
Ms. Zeng had a goal – living life to the fullest. She had resources – youth and family support. She was taking steps toward that goal by becoming fiscally responsible and spending more quality time with her family. She strove to maintain some control over her life – planning to work part time. Last, but not least, she had learned to let go of the past (“what I have done to deserve such a turn in my fortune”), treasure the present (one life and only one), and look ahead to the future, expecting a garden in full bloom after her labor.
Christian Theology of Hope
Dominican theologian, Aidan Nichols, has provided one of the best definitions of theology in my opinion. He contends that theology is a disciplined exploration of divine revelation. “Theology…provides one of the richest veins of ore in exploring what Christians mean by ‘revelation.’” [54] “The aims of the exploration will be those set by tradition, but the means…will be those of present-day…theory.” [55] Theology focuses on divine revelation, the personal self-disclosure of the divine to humankind. It is disciplined because it is grounded in Scripture and tradition. It is exploratory because it is not just a matter of repeating what past generations have said. Theologians know this, because every articulation of theological truth stands in the context of its time in history. Consequently, every generation must bring its questions and concerns to bear upon the theological process. While the basic truths do not change, our understanding does grow and develop. It is the Christian theology of hope that I will turn my attention to in the following discussion.
Grounding in Scripture. Hope in the Scripture of Judeo-Christian faith generally denotes a trust in God, the object of hope. It involves waiting patiently upon God, seeking what God has promised, or simply desiring and expecting something or someone to provide one with certain benefits in the future. [56]
There are several Hebrew verbs that may in certain contexts be translated “to hope” in English. One of them, qāwâbāt, denotes “hope” in the sense of “trust or wait hopefully” as when Jeremiah addresses God, “We wait hopefully in You” (Jer. 14:22). He also uses a noun formed from this root qāwâbāt (ךָוֶיקֹ֭) to teach that the LORD or Jahweh in Jewish is the hope of Israel (Jer. 14:8; 17:13; 50:7), which means that Israel’s God is worthy of trust. Another noun from the same root, ḇā-ṭaḥ-tî (בָ֭טַחְתִּ)meaning trust, is often also translated “hope” meaning “trust.” Similarly, the verb ḇā-ṭaḥ-tî(בָ֭טַחְתִּ)means “rely” in Psalm 25:2–3. [57]
For much of the Old Testament period, hope was centered on this world: the beleaguered hoped to be delivered from their enemies (Ps. 25); the sick hoped to recover from illness (Isa. 38:10–20); and Israelites trusted God to provide land, peace, and prosperity. In early passages there are few expressions of hope for the next world: those who descend to the grave have no hope (Isa. 38:18–19); only those still living could hope(Eccles. 9:4–6). Salvation was understood as deliverance in this life. In Deuteronomy 30:19, the choice between life and death is made clear, “See I have put before you today life and death, blessing and curse, and you shall choose life so that you and your seed shall live.” The choice is not whether or not to destroy one’s life but how best to live it.
However, this does not mean that the Israelites had no conception of, or beliefs in, a state of being beyond death. Robert H. Charles recognizes that early Israelite thought attributed a “comparatively large measure of life, movement, knowledge and, likewise, power to the departed in Sheol” and contends that the Israelites were hardly destitute of all notions of a future state. [58] Toward the end of the Old Testament, hope became more focused on the next world, especially on the resurrection. God made known His plan to bring His everlasting kingdom to earth (Dan. 2:44; 7:13–14) and to raise the dead (Dan. 12:2). God will “swallow up death forever” (Isa. 25:7), and the dead will rise again (Isa. 26:19); this hope of resurrection is the salvation for which the faithful wait (Isa. 25:9). The hope of immortality is connected to a religious faith, and it involves a soul [59] within a body, like that of Enoch (Gen. 5:24) or Elijah (2 Kings 2:11). [60]
The New Testament consistently uses the verb elpizō and the noun elpis for hope. [61] Hope comes as a gift from God through grace (2 Thess. 2:16). Just as the Old Testament emphasizes hope as trust, the Apostle Paul writes “our hope is in the living God” (1 Tim. 4:10) and “on Christ” (Eph. 1:12). As Jeremiah proclaims that God is the hope of Israel, Paul announces that “Christ Jesus our hope” (1 Tim. 1:1). The power of the Holy Spirit also causes hope to abound (Rom. 15:13).
Christians believe that the God who creates and sustains is primarily characterized by love, agape. The creation and the incarnation reveal the nature of this divine self-giving love. Christ is the visible expression of God’s faithfulness and gives every believer a reason to hope for the not-yetness in the future. This God who loves is trustworthy and keeps promises. God’s love is steadfast despite human rejection. Because of this, Christians can trust God with their future.
As the Lord told Jeremiah, “For surely I know the plans I have for you … plans for your welfare and not for harm, to give you a future with hope” (Jer. 29:11). Parallel to this, Apostle Paul says “hope does not disappoint us” (Rom. 5:5). The reason is that Christians already have a foretaste of the future glory because of “the love of God through the Holy Spirit which is given to us.” In other words, God’s gifts of love (through the Holy Spirit) are down payments of future glory for which Christians hope (Rom. 5:2; cf. Eph. 1:13–14).
The word “hope” is not very frequently seen in the Gospels, but the idea of looking expectantly is. Simeon looked for Israel’s consolation at the advent of the Messiah (Luke 2:25–26). Likewise, Anna, the prophetess, upon recognizing who Jesus was, proclaimed him to all those who were anticipating redemption (Luke 2:36–38).
In connection with hope in Romans 8:18–25, Apostle Paul speaks of waiting with eager expectation for the revelation of the adoption as children of God (v. 23), waiting “for the righteousness for which we hope” (Gal. 5:5) and for “the blessed hope,” namely, “the glorious appearing of… our Savior Jesus Christ” (Titus 2:13). Apostle Paul has both an eager expectation and a hope for God to be glorified in him, whether in life or death (Phil. 1:20). He goes on to express his desire to leave this world to be present with Christ (Phil. 1:23).
As hope is connected with patient endurance in the Old Testament, so in the New Testament trials lead to hope (Rom. 5:3–4) and hope is steadfast (1 Thess. 1:3; Heb. 3:6). When we hope for something we wait for it through patience (Rom. 8:25; cf. 15:4).
In the Old Testament hope is linked with “putting confidence in” God’s promises [62] or “taking refuge in.” Apostle Paul also parallels hope with trust. He hopes to send Timothy first and “trusts in the Lord” that he himself will come shortly (Phil. 2:24). Likewise, Apostle Paul links hope and boldness (2 Cor. 3:12). In a passage about the assurance of God’s promises, Hebrews 6:18–19 mention taking refuge by “seizing the hope set before us…an anchor of the soul.”
Reminiscent of the Old Testament false objects of hope, Apostle Paul counsels the wealthy not “to set their hope in wealth” (1 Tim. 6:17). In addition to putting hope in God and Christ, there is also hope for salvation (1 Thess. 5:8); for God’s glory (Rom. 5:2; Col. 1:27); for resurrection (Acts 23:6; 24:15; 1 Thess. 4:13); for the “redemption of our bodies” (Rom. 8:23); for righteousness (Gal. 5:5); for eternal life (Titus 1:2; 3:7); for the glorious coming of Jesus Christ (Titus 2:13); and for Christ’s Second Coming so that “we shall become like Him” (1 John 3:2–3). [63]
From the above list it is apparent that, in contrast to the Old Testament, New Testament hope is primarily eschatological. After being introduced late in Old Testament times, hope in the resurrection of the dead grew in the inter-testamental period in such proportion that Apostle Paul could speak of the resurrection as the “hope of Israel” (Acts 28:20; cf. 24:15; 26:6–8). The Christian hope is in the future. If hope is only for the present existence, it is most pitiable (1 Cor. 15:19). When fellow Christians die, believers grieve in hope of the Lord’s return, unlike unbelievers who have no hope. They believe that when Christ returns, believers, dead or alive, will be given imperishable bodies like that of the Risen Lord (1 Cor. 15:20–23, 51–52; 1 Thess. 4:13–18).
Hope is also the proper response to the promises of God. Christian hope is a hope “against all hope.” “Against all hope, Abraham in hope believed” (Rom. 4:18). Like Abraham, believers trust in God’s promises and seize “the hope set before us” (Heb. 6:18). Consequently, hope leads to joy (Rom. 12:12); boldness (2 Cor. 3:12); faith and love (Col. 1:4–5); fruitful labor (1 Cor. 15:51–58); comforting knowledge of resurrection (1 Thess. 4:18); exultation in sharing God’s glory (Rom. 5:2; cf. Heb. 3:6) and becoming pure “just as he (Christ) is pure” (1 John 3:3).
Ultimately the foundation of hope in the Christian tradition is rooted in the character of God, the object of hope. The covenant reveals God’s character, confirmed by God’s mighty acts. The followers of Jesus Christ perceive further revelation about the nature of God. Their hope is based on the truths about God’s character as revealed in the life, death, and resurrection of Jesus Christ.
Contemporary Theology of Hope. In the late 1960s, much of Christianity (if not most) was headed for some form of “Christian atheism” with a “God is dead” theology. A new school of German theologians came to the fore to refute it, propounding what has been variously termed the theology of hope or the theology of the future. [64] The pillars of this school are Jürgen Moltmann (Reformed), Wolfhart Pannenberg (Lutheran), and Johannes Metz (Roman Catholic). [65] It seeks to point theology toward the future, rather than toward the past or present. It places a strong emphasis on faith as it relates to history, but insists that the meaning of history can be uncovered only in its conclusion.
This theology of hope is grounded in the eschatology of Albert Schweitzer from the early twentieth century. In the words of Stephen Smith, Jürgen Moltmann “speaks of an understanding of God as being ahead of us, and the One who will make all things new. He (God) is known now in his promises… a world vividly aware of the ‘not yet’ dimensions of human and social existence, and of the fact that hope at its human level is of the stuff of meaningful existence.” [66] The present is understood as being meaningful only inasmuch as it relates to future possibilities. Christian hope lies in the anticipation of the historical future which will be a direct fulfillment of God’s promises as given to humanity in Christ, God’s Word incarnate. Similarly, Wolfhart Pannenberg speaks of the kingdom of God as the “eschatological future brought about by God himself,” [67] but he does caution that the futurity of God’s kingdom should not be taken to suppose that God is only in the future, and not in the present or the past. “Quite to the contrary, as the power of the future he dominates the remotest past.” [68] Johannes Metz sees the incarnate Christ establishing the kingdom of God by standing up for the outcasts of society and by preaching the coming kingdom of God as “the liberating power of unconditional love.” [69]
This theology of hope is also a resurrection theology. Christ’s resurrection as the “first-fruit” of the future is the beginning and promise of that which is yet to come. The promise of God, as evidenced by Christ’s resurrection, is analogous to the locomotive as a propulsive force of history. It awakens hope in those who are heavily laden. This hope is founded on faith in Christ, and it is this hope that is the “source of continual new impulses toward the realization of…freedom… in the light of the promised future that is to come.” [70] Johannes Metz believes that only on the basis of imminent anticipation of Christ’s Second Coming can one truly follow Christ and fulfill the social and political responsibilities expected of a Christian.
Like Marxism, the theology of hope goes beyond traditional theological bounds, seeking to envelop the whole world, including the fields of politics, sociology, ethics, and biology. It considers itself to be a theology of the secular culture and, as such – like Marxism – has had a definite impact on Third World thinking.
Critique. This school of German theologians focuses overwhelmingly on the future when God’s promises will be fulfilled. This may prompt a believer to ask, “Is my God a God of the future? If my hope is tied to the future, what is there for me to live for now?” “Is His kingdom a kingdom yet to come?” Stephen Smith’s comments provide a sobering thought:
“Is this theology no more than a sign of the times? Because our materialism and narcissism have blinded us to God as a living presence, have we now conjured a theology to somehow account for this by putting him into the future? Has virtue (hope) become the child of tragic necessity?” [71]
In his more recent book, In the End – The Beginning, Jürgen Moltmann responds to these questions by clarifying his theological position further. By saying that “Jesus is in the process of coming,” [72] he is saying that hope allows us to open ourselves today with all our senses for the experiences of Jesus’ arrival. Thus, even though God meets men and women out of the future, God is revealed in our past history and walks with us here and now. In other words, our hope in God gives us meaning for the present. Furthermore, Jürgen Moltmann affirms the fact that the kingdom of God is already “at hand” through Jesus, even though it is yet to be consummated. It has come to us already. We do not have to wait for it. We can already seek its righteousness and make it the goal of what we do in the world.[73] The Christian doctrine of hope is based on the remembrance of the coming, the death on the cross and the resurrection of Jesus Christ, as well as his Second Coming in the future.[74] This hope starts from a particular historical reality, and anticipates the future of that reality: its power over the future, and its consummation. I agree with him.
This theology of the secular culture also prompts one to ask: are we not rushing too hastily to change the world rather than changing ourselves first? In Time Invades the Cathedral, Walter Capps suggests that one of the weaknesses of this “theology of hope” school is that it fails, by and large, to address the question of the self. While its failure to do so is understandable given its concern to call attention “to the…Christian’s proper interest in caring for the world,” [75] Walter Capps notes that “in an age of transition, questions about the self emerge in an almost overwhelming way.” [76]
In my opinion, Jürgen Moltmann addresses this need for hope in personal transitions very elegantly. [77] He contends that it is in the creative expectation of Christ’s Second Coming that our everyday experiences of life’s transitions take place. We wait and hasten; we hope and endure; we pray and watch; and we are both patient and curious. In other words, we live in faith and with the hope that another world is possible. This makes Christian life exciting and alive and Christians enduringly capable of future. In asserting that Christian hope is a “hope against hope,” or a hope where there is nothing else left to hope for, Jürgen Moltmann speaks as if he is speaking to the terminally ill with unending misery. Through the power of hope, we do not give up, nor give ourselves up. We stay the course and remain enduring in a dark and deadly world. Such is the consoling and resisting power of hope.[78] I heartily agree.
However, little attention has been given by Jürgen Moltmann to the celebration of life or humor as the necessary companions of the struggle for continuing existence at the present. Jürgen Moltmann’s focus on hope seems strong on faith, but weak on love. After all, the creation and the incarnation of Jesus Christ reveal the very nature of God’s love. Love holds the key to transforming the self as well as the world. That is why the Apostle Paul said in 1 Cor.13:13, “we still have faith, hope, love, these three; and the greatest of these is love.
Jürgen Moltmann also does not say much about judgment and condemnation in his theology of hope. He perceives sin as a separation from God, and from the life God gives, [79] but does not say how the fall of humankind or human limitedness fits in with his theology of hope. What would happen if a terminally ill Christian with intractable pain opts for Physician Assisted Suicide? Is this considered a sin? Can this Christian still have the hope of resurrection and eternal life? In the Bible, resurrection can be unto either life (first resurrection) or condemnation (second resurrection). If so, which one will it be? These are questions I struggle with. I believe that God is a loving God and would see to it that we will not be burdened beyond what we can bear, and that “he who endures to the end will be saved” (Matthew 10:22, KJV). I agree with Jürgen Moltmann that our faith and hope in God will guide our Christian living. As for eternal life, I understand that we can have assurance of eternal life, but who are we to say that a person cannot be saved? Only God saves. God alone determines that.
I also agree with Jürgen Moltmann in our responsibility as Christians to fight against conditions which are in obvious contradiction to the kingdom of God and its righteousness. To help usher in the kingdom of God is not a vice of our presumption. As we cling to our hope in God, God has exalted us and invited us to transform our world in love and compassion. [80] The kingdom of God is not just God’s affair; it is ours as well.
Ellen Marshall, in her book Though the Fig Tree Does Not Blossom: Toward a Responsible Theology of Christian Hope, joins with Jürgen Moltmann in affirming this. “In order to accomplish its task, hope must be rooted in a relational concept of power that generates and sustains moral agency with its assertion that a flourishing whole is a collaborative endeavor and requires our participation.” [81]
Pastoral Theology of Hope
A discussion of theology of hope will not be complete without considering theology of hope from a pastoral perspective. The word “pastoral” may reflect different understandings in different contexts. In the present context, it refers to religious care for persons, families and communities.[82] A pastoral theology of hope is considered here as a form of theological reflection in which pastoral experience serves as the context for the critical development of basic theological understanding of hope that will inform all pastoral functions. [83] Through this theological lens, practitioners of pastoral care and counseling can better organize an effective pastoral response to ultimate concerns such as meaninglessness, isolation, groundlessness, and death.[84]
Nearly three decades ago, Robert Carrigan challenged pastoral theologians and pastoral counselors by pointing out the vital role that hope plays in pastoral care and counseling. As he observed, “In the face of all this new attention given to hope by theologians, philosophers, psychotherapists, and psychologists, it seems strange that there has been little or no attention given to the phenomenon of hope by pastoral theologians and counselors.” [85]
He was referring to the work of the theologians of hope (Jürgen Moltmann, Wolfhart Pannenberg, and Johannes Metz) who were then publishing important works on the future dimensions of faith and the centrality of hope and eschatology for Christian theology. Jürgen Moltmann, for example, was taking the stance that the basic identity of a person is hidden and can be revealed only by those unseen possibilities that lie beyond the future horizon. Human beings are “always on the way towards some … expected future whole.”[86]
Robert Carrigan wisely reminds us that God is involved in the present from both a past and future perspective. What God has done and will do are both represented in God’s presence and activity in the “eternal now.” Biblical concepts of time connect past and future to the present.Both history and eschatology are seen and experienced in the here and now. “Hope binds time and unites past and future in the present,” says Robert Carrigan. “Hope…is a here and now experience that contains both ‘first fruits’ that can be tasted now and a pledge of ‘things to come.’” [87]
Given the suffering of parishioners, patients and clients that is routinely faced by pastors, chaplains, and pastoral counselors as they minister to people who are drowning in despair, Robert Carrigan wondered, “Why is it that those of us in pastoral theology are not dealing with so important a topic (hope)?” [88] Regrettably, the pioneering work of Jürgen Moltmann, Robert Carrigan and others has had little impact on the literature in pastoral care and counseling for a good length of time.
It was not until 1995 when Andrew Lester published his book Hope in Pastoral Care and Counseling that hope was brought to the fore in pastoral theology. In Andrew Lester’s opinion, a basic reason for the subject of hope being neglected in pastoral theology is that the discipline of pastoral care and counseling has been taught and practiced under the worldviews of the social and behavioral sciences. [89] A psychoanalytic worldview has led us to appreciate the influence of the past on human personality. [90] We have also learned more about the significance of present circumstances on any person’s life situation from social learning theories, cognitive theories, systems theories, etc. However, the fact that humankind is constantly moving into the future dimension of temporality has been largely neglected. In Andrew Lester’s opinion, equal emphasis for the future dimension is necessary for a more holistic psychological and theological understanding of what Anton Boisen called “the living human document.” [91] Pastoral theology of hope may well provide a theological lens through which practitioners of pastoral care and counseling can better organize an effective pastoral response to human suffering and despair.
In proposing a pastoral theology of hope, Andrew Lester is proposing a paradigm shift: (1) like the other German theologians of hope, Andrew Lester has incorporated into his pastoral theology the future dimension of temporality in the practice of pastoral care and counseling; and (2) he proposes to build his theology on theological anthropology.[92]
John Macquarrie once said, “It has been my contention for a long time that the doctrine of persons is the right starting point for a contemporary theology.”[93] What he meant was that the human condition should inform theological insight, especially when each person faces life’s inevitable and irrational pain and suffering. This human condition may include one’s identity (essence or “substance of being”[94]), personality, self (consisting of body, spirit and soul), [95] or experiences (in terms of feelings, thoughts, concerns, desires as well as the outside world of events and people).
Wolfhart Pannenberg further reminds us that “Christian theology in the modern age must provide itself with a foundation in general anthropological studies,” [96] human studies that include humanities (such as philosophy, religion, history, languages, arts and literature) and social sciences (such as psychology, sociology, anthropology, cultural studies and economics). He points out that understanding human interaction with the world, in both itsphysical and cultural aspects, should be the foundation for theological reflection. Any explanation or defense of our faith must be fought “on the terrain of the interpretation of human existence.”[97]
Andrew Lester followed the suggestions of John Macquarrie and Wolfhart Pannenberg by starting out with theological anthropology. He argues that modern theologians, including pastoral theologians, must begin their enterprise with an anthropological foundation for understanding religious experience. He hopes that pastoral theology, at its best, can allow mutual critique between knowledge generated by the human sciences on the one hand and the wisdom of the Christian tradition on the other. Perhaps the integration of theories and theology in praxis (alternating reflections and actions) may prove to be helpful in providing care to those suffering in despair.
Andrew Lester has identified a number of anthropological building blocks for his pastoral theology of hope: [98] (1) time-consciousness must be recognized as a basic component in human existence; (2) future tense is a primary dimension of this temporality; within this context, meaning and purpose in life can be realized; (3) human beings are storied creatures who, through narrative principles, develop core narratives that structure their sense of self-in-the-world; [99] (4) future stories are basic elements in these core narratives; and (5) all human brokenness is inescapably connected to disturbances in future dimensions of temporality. Andrew Lester points out that, although our past experience shapes our responses (to crisis, grief, anxiety, etc), the awareness of our future being threatened or already changed will create the actual pain and suffering. He maintains that human brokenness is linked inseparably to problems with our future projections. A major aspect of that brokenness has to do with the disruption, or the loss, or the failure of our future stories.
Summary and Discussion
Hope is an intuitive perception with the enduring belief that something or someone will provide a future realizable good. This hope can be either gifted by God as a virtue, or acquired as an attitude of strength (fortitude) in a mutually trusting relationship, and developed with active seeking. Hope is verified in its origin by the “internalization” of a “transitional object,” and in its development by the outside world. Hoping is a process that requires awareness of possibilities and difficulties, as well as active engagement toward achieving a goal. The allies of hopefulness are enduring trust, patience, and modesty (with willingness to let go). Its enemies include despair, apathy, and shame against which hope can be dashed. Its fulfillment brings satisfaction to one’s persistent longing. Hoping is an experiential process that rests in meaning, giving the terminally ill reason for living. Hoping is also a relational process that rests in love, requiring communal support; a spiritual process that rests in faith and spirituality, empowering the hopeful; and a rational process that rests in thoughts and actions, prompting one to move forward in the achievement of a realizable good. Hope does not speak to us only in the future. Its impact is on the present, the here and now.
As an attitude and a disposition, “hope must be practiced because it is essential to daily life, the moral life…” and spiritual life as well, and “because responsible hope does not come naturally.” [100] “Given the often overwhelming experiences of life, we must frequently practice hope in pieces, sometimes grieving and shouting, sometimes celebrating,” “attending to possibilities and to limitations. It (hope) buoys the spirit and steels the spine.” [101] In the next chapter, we will see how this knowledge contributes to the fostering of hope in matters of existential concern.
[1] Interview #10, Appendix.
[2] William B. Nelson, Jr., “Hope,” Evangelical Dictionary of Biblical Theology, ed. Walter A. Elwell (Grand Rapids, MI: Baker Book House, 1996), 355.
[3] St. Thomas Aquinas, Summa Theologica, trans. Wilfrid Lescher, vol. 2 (London: Thomas Baker, 1906), Q. 17, Art. 1.
[4] Charles R. Snyder, The Psychology of Hope: You Can Get There From Here (New York: Free Press, 1994), 5.
[5] Lester, Hope in Pastoral Care and Counseling, 62.
[6] Erikson, “Human Strength and the Cycle of Generations,” 118.
[7] Donald Capps, Agents of Hope: A Pastoral Psychology (Minneapolis: Fortress Press, 1995), 52.
[8] Ray S. Anderson, Spiritual Caregiving as Secular Sacrament: A Practical Theology for Professional Caregivers (London: J. Kingsley Publishers, 2003), 145-62.
[9] M. Cathleen Kaveny, “Cultivating Hope in Troubled Times” [online]. Lumen Magazine (University of Notre Dame, November 2005), http:// www.nd.edu/~lumen/2005_11/CultivatingHopeinTroubledTimes. shtml (accessed May 25, 2008).
[10] Erikson, “Human Strength and the Cycle of Generations,” 111-57.
[11] Ibid., 115.
[12] Erikson, “Human Strength and the Cycle of Generations,” 118.
[13] Capps, Agents of Hope, 98-136.
[14] Erikson, “Human Strength and the Cycle of Generations,” 118.
[15] Ibid., 115.
[16] Erikson, “Human Strength and the Cycle of Generations,” 117.
[17] Ibid., 116. The egois the “I,” the center of consciousness, an entity comprising everything a person believes himself or herself to be, including thoughts, feelings, wants, and bodily sensations. According to Carl Jung, the ego mediates between one’s unconscious realm and the outside world.
[18] Ibid.
[19] Ibid., 117.
[20] Erikson, “Human Strength and the Cycle of Generations,” 117.
[21] Ibid., 116.
[22] Erik H. Erikson, Identity: Youth and Crisis (New York: W.W. Norton, 1968), 216-21.
[23] W. Clifford M. Scott, “Depression, Confusion, and Multivalence,” International Journal of Psychoanalysis 41 (1960): 497-503.
[24] Paul W. Pruyser, “Maintaining Hope in Adversity,” Pastoral Psychology 35 (1986): 123.
[25] Paul W. Pruyser, “Phenomenology and Dynamics of Hoping,” Journal for the Scientific Study of Religion 3 (1964): 86-96.
[26] Interview #7, Appendix.
[27] Erikson, “Human Strength and the Cycle of Generations,” 117.
[28] Paul W. Pruyser, The Play of the Imagination: Toward a Psychoanalysis of Culture (New York: International Universities Press, 1983), 19.
[29] Pruyser, Play of the Imagination, 19.
[30] Erikson, “Human Strength and the Cycle of Generations,” 117.
[31] Interview #15, Appendix.
[32] Interview #1, Appendix.
[33] Interview #9, Appendix.
[34] Interview #17, Appendix.
[35] “On Utopia,” Chap. 9 in Liji 禮記: The Book of Rites [in Chinese], a Confucian classic believed to be edited by Confucius (Jinan, Shandong: Shandong Friendship Press, 2000).
[36] Bowman and Singer, 455-64.
[37] DeGraff (a.k.a. Thanissaro Bhikkhu), “Life Isn’t Just Suffering.”
[38] Lao-zi, Tao Te Ching, Chapter 58. See also Yu-hsi Chen, “TheWay of Nature as a Healing Power,” Handbook of Multicultural Perspectives on Stress and Coping, ed. Paul T. P. Wong and Lilian Wong (New York: Springer, 2006), 92.
[39] Lao-zi, Tao Te Ching, Chapter 13.
[40] Farran, Herth and Popovich, Hope and Hopelessness, 6.
[41] Frankl, Man’s Search for Meaning, 75.
[42] See story from Interview #10, Appendix.
[43] Nietzsche, “Twilight of the Idols,” 9:8.
[44] Jean Nowotny, “Despair and the Object of Hope,” The Sources of Hope, ed. Ross Fitzgerald (Rushcutters Bay, Australia; Elmsford, NY: Pergamon Press, 1979), 66.
[45] Ibid., 57.
[46] Ibid.
[47] Gabriel Marcel, Homo Viator: Introduction to a Metaphysic of Hope (Gloucester, MA: Peter Smith, 1978), 10.
[48] Schubert Ogden, “The Meaning of Christian Hope,” Union Seminary Quarterly Review 30 (winter-summer 1975): 159.
[49] Abraham Heschel, The Prophets (New York: Harper & Row, 1962), 96-97.
[50] Anderson, Spiritual Caregiving as Secular Sacrament, 145-62.
[51] Erich Fromm, The Revolution of Hope: Toward a Humanized Technology (New York: Harper & Row, 1968), 14.
[52] Farran, Herth and Popovich, Hope and Hopelessness, 9.
[53] Story from Interview #12, Appendix.
[54]Aidan Nichols, The Art of God Incarnate : Theology and Image in Christian Tradition (London: Darton, Longman and Todd, 1980), 105.
[55] Ibid., 89.
[56] Nelson, “Hope,” 355.
[57] Ernst Hoffman, “Hope” in Dictionary of New Testament Theology, ed. Colin Brown, vol. 2 (Grand Rapids, MI: Zondervan, 1976), 239.
[58] Robert H. Charles, A Critical History of the Doctrine of a Future Life in Israel, in Judaism, and in Christianity (London: A. & C. Black, 1899; reprint, Whitefish, MT: Kessinger Publishing, 2007), 41.
[59] Soul is defined here as the animating center of a person’s life. It is also believed to be the seat of relatedness to the divine.
[60] S. D. F. Salmond, Christian Doctrine of Immortality, 3rd ed. (Edinburgh: T. & T. Clark, 1897), 159.
[61] Hoffman, “Hope,” 238.
[62] Walther Zimmerli, Old Testament Theology in Outline, trans. David E. Green (Atlanta: John Knox Press, 1978), 31.
[63] Paul S. Minear, Christian Hope and the Second Coming (Philadelphia: Westminster Press, 1954), 101.
[64] Some theologians wish to dichotomize these terms into two separate schools of theological thought, but they have enough similarities to retain them as a single entity.
[65] David L. Smith, A Handbook of Contemporary Theology (Wheaton, IL: Victor Books, 1992), 135-49.
[66] Stephen M. Smith, “Theology of Hope,” in Evangelical Dictionary of Theology, ed. Walter A. Elwell, 2nd ed. (Grand Rapids: Baker Book House, 2001), 577.
[67] Wolfhart Pannenberg, Theology and the Kingdom of God, ed. Richard J. Neuhaus (Philadelphia: Westminster Press, 1969), 53.
[68] Ibid., 62.
[69] Johannes B. Metz, Faith in History and Society: Toward a Practical Fundamental Theology, trans. David Smith (New York: Seabury Press, 1980), 90.
[70] Jürgen Moltmann, Theology of Hope; On the Ground and the Implications of a Christian
Eschatology, trans. James W. Leitch (New York: Harper & Row, 1975), 22.
[71] Stephen M. Smith, “Hope, Theology of,” 578-79.
[72] Jürgen Moltmann, In the End, the Beginning: The Life of Hope, trans. Margaret Kohl (Minneapolis, MN: Fortress Press, 2004), 89.
[73] Ibid., 92.
[74] Ibid., 88.
[75] Walter H. Capps, Time Invades the Cathedral: Tension in the Schools of Hope (Philadelphia: Fortress Press, 1972), 134.
[76] Ibid., 137.
[77] Moltmann, In the End, the Beginning,94.
[78] Ibid., 90.
[79] Moltmann, In the End, the Beginning, 93.
[80] Ibid., 94.
[81] Marshall, Though the Fig Tree Does Not Blossom, 97.
[82] Taken from the Mission Statement of the Society of Pastoral Theology, accessed 4 April, 2009; available from www.geocities.com/societyforpastoraltheology/aboutspt.html.
[83] J. Russel Burck and Rodney J. Hunter, “Pastoral Theology, Protestant,”in Dictionary of Pastoral Care and Counseling, ed. Rodney J. Hunter (Nashville, TN: Abingdon Press, 1990), 867.
[84] Yalom, Existential Psychotherapy, 8.
[85] Robert L. Carrigan, “Where Has Hope Gone? Toward an Understanding of Hope in Pastoral Care,” Pastoral Psychology 25, no.1 (Fall 1976): 39.
[86] Moltmann, Theology of Hope, 286-87.
[87] Carrigan, 49.
[88] Carrigan, 40.
[89] Lester, Hope in Pastoral Care and Counseling, 21-22.
[90] Personality is defined as the totality of one’s behavioral and emotional characteristics in Merriam-Webster Dictionary.
[91] Anton T. Boisen, The Exploration of the Inner World: A Study of Mental Disorder and Religious Experience (New York: Harper & Brothers, 1952). The phrase “human document” is Boisen’s way of reminding us that any human being is a unique text that must be read (heard) and interpreted (the hermeneutical task).
[92] Lester, Hope in Pastoral Care and Counseling, 23.
[93] John Macquarrie, “Pilgrimage in Theology,” Epworth Review 7, no. 1 (January 1980): 47-52.
[94] Karl Barth, Church Dogmatics, vol. 2, pt. 1, trans. G. T. Thomson (Edinburgh: T & T. Clark, 1957), 287-97.
[95] Anderson, Spiritual Caregiving as Secular Sacrament, 25.
[96] Wolfhart Pannenberg, Anthropology in Theological Perspective, trans. Matthew J. O’Connell (Philadelphia: Westminster Press, 1985), 15.
[97] Pannenberg, Anthropology in Theological Perspective, 15.
[98] Lester, Hope in Pastoral Care and Counseling, 56.
[99] Similar to Georg Hegel’s “being-in-itself,” or “essence,” a nature that is fixed and immutable.
[100] Marshall, Though the Fig Tree Does Not Blossom, 107.
[101] Ibid.
CHAPTER 5: Is Fostering Hope Justified in the Terminally Ill?
Ethical Consideration
Does fostering hope [1] conflict with the terminal patients’ acceptance of death?James Greek asks a probing question regarding the care of the terminally ill: “Do we approach them and their families with hope, or do we put on ‘an emotional neutrality’ in the name of acceptance that can be interpreted as hopelessness?” [2]
Before we try to answer this question, it is important to know what form of acceptance is present in the terminally ill. Acceptance can be an enthusiastic welcoming, a grudging resignation, or a variety of other responses, including sadness or an inner peace.[3] It is important for the caregiver to listen actively to, and feel with, the terminally ill as they manifest their individual responses of acceptance and their true needs. When the dying person welcomes the imminence of death, there is hope in resting from earthly labor and from pain and suffering as well as, for religious persons, celebrating the joy of joining the transcendent One. As the Apostle Paul says, “To die is gain” (Phil. 1:21). When the acceptance is accompanied by a grudging resignation, there is even more reason for hope, the hope of seeing children grow up, daughter getting married, grandchild being born, and a long lost brother come home. When there is sadness over separation from loved ones, there can be hope for a joyful reunion someday. Even when acceptance brings with it inner peace, there is once again the hope of spending every waking moment with one’s beloved. Indeed, where there is life, there is hope. We remain hopeful even when we do not attain what we hope for. Even as certain hoped-for events are coming to pass, they have already been quietly superseded by a more advanced set of hopes. Our object of hope can be defined and redefined time and time again. This hopefulness is intrinsic to who we are.
Acceptance was listed as the last stage in Elizabeth Kübler-Ross’s proposed model of coping with dying [4] as if acceptance were the end of one’s coping. Many clinicians who work with the dying have found this to be misleading.[5] Even with acceptance, there are more fundamental existential questions to consider – questions like “How shall I live? How can I rise above the darkness that engulfs me?” Paul Wong tells us,
“Acceptance can be the beginning of positive growth, with adaptation to tragic circumstances and striving for the best out of one’s life within these constraints. It can mean wisdom of expecting the worst, hope for the best, and preparedness for whatever that comes. It can herald the indomitable human spirit to shine in the darkest of nights.” [6]
This growth involves embracing the bad through positive acceptance, and discovering the good through affirmation. Acceptance is positive when it accepts the negative without losing faith in the positive. Viktor Frankl, founder of logo-therapy, contends that even in the most horrible circumstances, one can still discover positive meaning, and maintain a sense of wonder at the beauty of nature and human dignity. [7] Lao-zi, the revered teacher of Taoism, observes: “Highest good is like water. Because water excels in benefiting the myriad creatures without contending with them and settles where none would like to be, it comes close to the Tao.” [8] In the broadest sense, “a Taoist attitude toward life can be seen in the accepting and yielding, the joyful and carefree sides of the Chinese character.”[9] No matter how tragic and despicable life can be, there is always sweet joy in positive acceptance. It is through hope that we can experience inner peace and joy even in the midst of adversities. It is through accepting life’s perils that we long for the promises, through tragedies that we see beauty, through suffering that we gain enlightenment, and through vulnerability that we find redemption.
The next question to be considered is: Does hope mean denial of reality concerning the care of the terminally ill? When the Imam found his mother’s life sustained on long-term life-support systems, he placed her in Allah’s hands. “I knew I was hoping against hope, but I kept telling myself that nothing is absolute. Miracles can happen.” [10] Is this denial of reality? Is hope for the miracle of physical recovery a denial, a failure to have achieved acceptance of reality, or is it a desperate attempt to cope with the impending loss of a loved one? If it is a mode of coping and it is making the son feel better at the moment, should he be deprived of this hope? Should he be confronted with “reality” forcefully and be deprived of his “illusions” even though uncertainty with possibility is his choice?
Merle Mishel, in her theory of uncertainty in illness, states, “Illusions are defined as beliefs constructed out of uncertainty – beliefs that are viewed in a particular light with emphasis on their favorable aspects.”[11] In other words, uncertainty can be viewed as favorable opportunity. How is this related to hope, especially the hope against hope? Merle Mishel attributes a process of “buffering” to this hope when coping with the unbearable. She states, “Buffering serves the purposes of blocking the input of new (unfavorable) stimuli that could alter the view of uncertainty as opportunity.”[12] Personally, I believe that miracles can happen and there is nothing wrong with wishing and praying for them. However, people’s lives must be helped to move on without depending on miracle cures.
Some patients prefer not to talk about their terminal illnesses.[13] Some evade the topic of death altogether, especially among Chinese. Does it mean that they are in denial of reality? Is it necessary to remind them of the seriousness of their illness? Like acceptance, denial can also describe a whole range of responses: (1) I am not ill; (2) I am ill, but it is not serious; (3) I am seriously ill, but not dying; and (4) I am dying, but death will not come for a long time. [14] Thus, when a patient denies that death is imminent, there may well be an acceptance already of the fact that s/he is dying. Why should it be necessary then to remind her/him of that fact?
Richard Lazarus, a longtime researcher and theorist on stress and coping, talks about the positive aspects of maintaining ambiguity. He provides the example of “a person with a terminal illness who won’t talk about it. That person is not necessarily denying the facts of the illness, but simply avoids talking about it as a means of self-protection. Constant discussion of an illness can discourage hope, and hope is needed when you recognize the situation is bad.”[15] Richard Lazarus mentions two functions of coping: regulation of emotional distress and problem solving. It seems likely that many health care providers focus on the problem solving while many recipients of care focus on the former instead, preferring to regulate the distress so that it does “not get out of hand” and “damage or destroy morale and social functioning.” They may “feel better…by denying, intellectualizing, avoiding negative thoughts, or taking drugs.” [16] Hence, if these recipients of care opt for uncertainty, it may be wise to err on the ambiguous rather than insist on the rational truth-telling. Inge Corless suggests that these two distinctive worldviews, one based on faith and hope, the other on positivism and scientific enquiry, can co-exist “in a creative synergy” instead of dominating over one another.[17] There should be room for the Muslim, Taoist, Buddhist, and Confucian (atheist) alike to choose for themselves uncertainty and possibilities. Instead of engaging the terminally ill in a dialogue about death, it may be wiser to engage them in a dialogue about life, giving them encouragement and support in maintaining normalcy for their daily tasks of living.
In conclusion, the author firmly believes that fostering hope in the terminally ill is ethically justified.
Existential Consideration
This second part of the chapter attempts to argue the fact that hope in its various dimensions is uniquely suited to deal with the existential concerns commonly found in the terminally ill. Irvin Yalom has identified four such existential concerns: meaninglessness, isolation, groundlessness, and death.[18] People become aware of these existential realities at various times in their lives, but nowhere more acutely than the end stage of their lives.
Facing existential concerns is sometimes called facing “the void.” [19] This can happen when one is afflicted with pain and suffering. Events such as cancer, bereavement, and other tragedies may lead to despair (hopelessness). “Seeing what havoc a disturbed person can cause with an assault rifle, visiting the oncology ward at a children’s hospital, walking through the museum at Dachau, hearing a trusted and loved spouse announce that she wants a divorce, attending the funeral of a doctor gunned down in his office – these are the life situations that raise questions about meaning and hope.” [20]
When people stare into the void, they may have one of two experiences. Some people encounter the transcendent One. Christianity affirms that God dwells even in this void. James Loder said that we may see in the void “the face of God,” the transcendent source of hope in the face of existential realities.[21] Sometimes however, people find the void filled with nothingness and hopelessness. It is a fearful experience. Many people have commented on the inadequate ways in which humans try to fight off meaninglessness, but few have talked about our ways of trying to cope with the hopelessness that is felt in the face of these existential realities.
Meaninglessness and Hopefulness
When one must inevitably travel the road of suffering unto death, one often wonders what possible meaning one’s life has. The terminally ill with intractable pain would be asking, “Why bother to live? How shall we live?” These questions are difficult to answer, as discussed in Chapter Three. Arguments abound as to whether or not there is a universal meaning to life, in contrast to it being entirely personal. If indeed “God is dead,” and there is no pre-ordained design or divine purpose in our lives, does it mean that we would have to construct our own meaning in life, or discover it through our heritage? Even though these questions sound philosophical and impractical, they are existential questions that the terminally ill have been asking.
Meaning and hope are related but different concepts. Both involve experiences (events, emotions, concerns and desires), support from others (relationships), spirituality (faith/belief), and rational thoughts (creative/insightful thinking or attitudes). [22] Both are very much influenced by culture, heritage, or community. However, as we have defined it in Chapter Three, meaning of life generally refers to a concept concerning the value or significance of life, while hope is more related to the purpose of life, with an anticipated goal that guides human actions in living. This hope, like the purpose of life, is related to a vision or projection of the future, but with an impact on the present, the here and now.
Hopefulness, unlike hope, is neither a concept nor a goal. It is an intuitive process of projecting into the future an enduring belief of achieving a realizable good. Unlike the will, hopefulness is the earliest virtue developed in infancy, and it (1) involves a persistent desire for (or a goal to) something good (even in the “paradoxical” hope of “good death” through Physician Assisted Suicide); (2) involves the use of resources to overcome difficulties ahead because of reality; (3) involves small steps toward the goal; (4) involves some kind of control by being able to shift alternatives in meaning and re-definition of objectives; and (5) involves actions and hard work, taking the concept of meaning and “running with it” to attain the goal. Based on these characteristics, hopefulness resting in meaning appears to be uniquely suited to help the terminally ill in living through their pain and suffering as they face meaninglessness.
Hopefulness Resting in Meaning.[23] This emphasis on meaning is not new. Viktor Frankl’s book Man’s Search for Meaning first brought this to our attention. Hope is not necessarily a belief that something is going to go well, but rather it is an enduring belief that whatever happens (in the future) will make sense, no matter how it turns out.[24] Debra Parker-Oliver sees hopefulness as the positive expectation for meaning attached to life events.[25] This definition does acknowledge a positive ideology, and nullify the idea of “false hope.” However, it argues that it is irrelevant as to whether what is hoped for can actually be achieved. Hopefulness lies in meaning that is attached to life, not in events themselves. This definition recognizes that individuals can shape their hopes by finding new meanings for living. This hope allows a form of control over events in life that feel uncontrollable. This hopefulness also sets personal goals, allowing individuals to become active participants rather than passive recipients of life events, being vulnerable to others’ definitions and meanings. Thus, as long as there is meaning, there is hopefulness. The key to hopefulness does not lie in life events, but in meaning created or discovered in these events.
Elizabeth Kübler-Ross, while working with the dying, wrote: “Watching a peaceful death of a human being reminds us of a falling star; one of the million lights in a vast sky that flares up for a brief moment only to disappear into the endless night forever.”[26] But, is that all to life, one may ask? The secular American culture does not believe that hope is at all possible for those who know they are dying. However, if hope is entrenched in meaning, and meaning is socially constructed, then fostering hope in the dying is justified. As the dying person searches for meaning, peace is more likely to be found.[27]
Cathleen Fanslow-Brunjes et al. suggest that hope in the dying can involve four phases: [28] a hope (1) for cure; (2) for treatment; (3) for prolongation of life; and (4) for a peaceful “good death.” Thus, the objective of hope can be changed, re-aligned, refocused, or redefined. It can take many forms, depending on the goals of the hopeful individual. The challenge for those working to foster hope in the dying is to help the dying create or discover meaning, which shines forth as that “brightness experienced before a star falls.” This should help to overcome the meaninglessness commonly found in the terminally ill.
Isolation and Hopefulness
In interpersonal life, the self is experienced as an openness of one’s soul to the life of others in a bond of mutual trust and support. This interpersonal life can relate to either God or others. Our identity is not so much determined by self-reflection as by intentions and actions through which the self is related to others. John MacMurray says it well: “I need you to be myself.” [29] Martin Buber, the Jewish philosopher who is most remembered for his classic treatise on the nature of the self as being personaland relational, wrote:
“The You encounters me by grace – it cannot be found by seeking…The basic word I-You can be spoken only with one’s whole being. The concentration and fusion into a whole being can never be accomplished by me, nor can it be accomplished without me. I require a You to become: being I, I say You.”[30]
As important as this relatedness may be, interpersonal isolation can arise when there is a gulf between oneself and others (including God). While there can be many reasons for such an alienation, an affliction with a terminal illness may be one of these reasons. The terminally ill may often retreat into a cocoon and isolate themselves from others, including the Divine. They may also feel as if their friends were avoiding them like the plague.[31]
A second form of isolation is intrapersonal isolation. It is a process whereby one partitions off parts of oneself. Freud used the term “isolation” to describe a defense mechanism, especially apparent in obsessional neurosis, in which an unpleasant experience is stripped of its effect, and its associative connections are interrupted, so that it is isolated from ordinary processes of thought.[32] In the contemporary psychotherapy scene “isolation” is used not only to refer to formal defense mechanisms but in a more casual way to connote any form of fragmentation of the self. Thus, intrapersonal isolation results whenever one stifles one’s own feelings or desires, accepts “oughts” or “shoulds” as one’s own wishes, distrusts one’s own judgment, or buries one’s own potential.
Existential isolation, however, cuts beneath these forms of isolation. No matter how closely we relate to another individual, there remains a final unbridgeable gap. Each of us arrives in this world alone and must depart from it alone. [33] In each individual, in the dawn of consciousness, is created an ego-self (transcendental ego) by permitting consciousness to curl back upon itself and to differentiate a self from the remainder of the world. This is a self that has an instinctive and existential “reach” for a transcendent reality.[34] According to Ben Mijuskovic, [35] there is a fundamental loneliness in all individuals, where one cannot escape the knowledge that while each of us “constitutes” one another (as posited by John MacMurray and Martin Buber), we can never fully share our consciousness with others.
It is not uncommon to find a terminally ill person retreat into isolation and set up defenses against any intrusion or interruption. The challenge for the caregiver is to overcome the effects of this constriction of the self and enable this person to emerge into a larger space of self-expression and relation with others. The Old Testament theologian Walter Brueggemann reminds us that “Hope emerges among those who publicly articulate and process their grief over their suffering.” [36] Instead of suppressing the pain, anger and grief, the bereaved would do well to articulate and process the grief and let hope emerge to liberate them and transform their suffering and losses into creative purpose for their re-engagement of life.
In her insightful treatment of the inexpressibility of physical pain, Elaine Scarry reminds us that pain can so narrow a person’s social and spiritual horizons that s/he loses a total sense of personal existence. Paradoxically, at the same time, pain fills the entirety of one’s existence so that those who seek to enter into that person’s existence can only do so through the window of pain. “Pain has the power to end all aspects of self and world.” [37] For all other sensations and feelings, usually there can be found an object or a language by which the feelings can be expressed. Pain is different, Elaine Scarry tells us. The person tends to isolate and silence the self.
Building on this thought, Stanley Hauerwas says, “Pain, in effect, is the enemy of community precisely because we cannot feel one another’s pain.”[38] Attempts to “get around” pain by either neutralizing it with pharmaceuticals or seeking to get at the physical source of the pain itself, says Stanley Hauerwas, may “alienate the patient from his or her own experience.”[39] Mr. Zhang was reluctant to take his pain relief medication, because he hoped to “remain relatively alert and enjoy quality time” with Ai Yi as much as possible.[40]
When we begin with a view of the self as intended by God to be free of pain and impervious to suffering, we end up with a caricature of both God and the human person. Ray Anderson cautions us that we should not view God as being so abstractly good and powerful that God no longer has a place in a world that is neither. [41] Similarly, the human self, when idealized, can no longer have any relevance for persons attempting to find their identity in the multiplicity of self-images.
In the face of the pervasive existential reality of pain and suffering, we face two temptations. One is to resign to the fact that pain and suffering are inevitable and certain, and that God is no longer sustaining us in the present as God has sustained us in the past. Another temptation is to mask the reality by inventing a coping mechanism of denial, or avoidance.
Paul Pruyser suggests that pretending not to see or to feel the pain and suffering is a form of avoidance and possibly not the best answer. He thinks that turning to future promises will only break us off from the real world, even though there may be a temporary relief from the anguish caused by intense pain. A better alternative may be to acknowledge and express one’s isolated situation in existence and confront this with resoluteness.[42] Maybe then one can respond to others’ love and concern with appreciation. If, on the other hand, one is so preoccupied with isolation that one cannot turn toward others, there is often a tendency to blame others as an excuse for one’s own isolation. In such an instance, what could have been an authentic relationship can become out-of-joint and distorted.
Paul Pruyser suggests that we go back to divine providence, viewing it “predominantly as Benevolence, whose benevolent intention will come through even in incalculable events and unforeseeable forms.” Citing psychoanalyst Ernest Jones’s observation that “what one really wants to know about the divine purpose is its intention toward oneself,” Paul Pruyser concludes that “the foremost discovery to be made (regarding divine providence) is that one must come to terms with benevolence,” and this means that “divine benevolence, like human benevolence, is a promise to be with us in trouble, to be present now (and not in the future) in our hours of agony, but not to perform magical cures and miraculous healings, to send forth angels of mercy…or to postpone the hour of our death.”[43] This is in line with what Lee Snook, a process theologian, proposes: “a Christian’s basis and object of hope is God’s faithfulness,” and “not an afterlife with a non-perishable body living in paradise” which we suppose has been guaranteed for us. “The future is neither predicted nor guaranteed by Christian faith,” but it is “a faithful God who in Jesus Christ has sealed His promise that no matter what that open future may bring us, we will not be separated from the love of God.”[44]
Hopefulness Resting in Love and Support. Stanley Hauerwas suggests that, when we do experience pain within a community of love and support, there is an interchange, a transfusion, so that what life flows out of us flows back into us, filtered through the fabric of intentional care.[45] Within the life of the self in relation to others, there flows the pain of others as well as the joy of others. The move toward health and healing through the creative power of the spirit takes place within the life of the community and the care which members have for one another, just as the Bible says, “…one member suffer, all the members suffer with it; or one member be honored, all the members rejoice with it” (1 Cor. 12:26 AV).
As we have discussed, hopefulness is a communal and relational process, not isolationist or separatist. People who can hope are people who are meaningfully connected with other people. Robert Beavers and Florence Kaslow observed that hopefulness “does not exist in a vacuum, but rather in shared experiences with others,” [46] hoping with or for others, which transcends the lone individual and his/her ego needs. “Community is the vehicle of hoping.” [47] Whether the community is one’s own family and friends, or a larger entity such as a nation or a church, the hopeful person feels a connectedness with it. We look for community in which to share hope and share visions of the future. William Lynch says, “Hope cannot be achieved alone. It must, in some way or other, be an act of a community.” [48] Despite the tendency to retrieve into a shell, the terminally ill need all the help they can get from others to encourage and support whatever hope is envisioned. The desperate need for hope in the face of hopelessness tends to push us toward relationships. Hopefulness rests in trust and love, just as we have seen how hopefulness originates in infancy. New or rediscovered friendship can open up the future and produce energizing hope: “When friendship is born, time begins to move again, and simultaneously hope awakens like a melody which stirs in the depths of memory.”[49] The reverse is also true: relationships that fall apart may contribute to a loss of hope. Grief over the loss of some important person often leads to a sense of hopelessness. This stresses the important role of the caregiver as a trusting person with unwavering commitment to the care of the terminally ill.
Hope can be discovered in a mutuality of trust and care. In mutual relationships each person is helping the other to gain interior freedom, to achieve individual identity, and to become fully autonomous within the connectedness of the relationship.[50] Some relationships are destructive to hope, particularly relationships in which one person dominates, abuses, uses or discounts the other. These non-mutual relationships make love conditional on obedience, submission, or dependence. The conditionality tends to make people feel trapped and stunts the process of individualgrowth and the development of hope. Terminating non-mutual relationships may be necessary because they foster despair rather than hope. Hopelessness tends to be suspicious of others and doubts whether other people can understand. Hopelessness pushes people into believing that other people would be better off without them. People infected by hopelessness are less likely to have meaningful relationships or a significant community.
For the person who is suffering, William Lynch wrote, “Perhaps it is impossible to really despair with someone else…perhaps it must be a private act.” [51] We have seen how people went into a shell when they suffer. Those in despair tend to close themselves off from others, and often do not feel deeply connected with anyone and are frequently without commitments to anything or anybody outside themselves. They tend to be isolated, alone, separated, disconnected, lonely, estranged, and/or alienated. This creates a Catch-22 situation, and unless a caring community takes the initiative to approach them in genuine friendship and love, the hopeless will remain disconnected and alienated. When friends or family members withdraw or close themselves off from us, we need to be alert and consider the possibility that they have begun to feel hopeless. Even though no relationship can eliminate isolation, relationship can be shared with another in such a way that thepain of isolation is assuaged.
Groundlessness and Hopefulness
While hope is closely associated with the positive formation of personal autonomy (starting from the second or early childhood stage of development), there is no denying that this new-found freedom can also create anxiety and fear. It is true that ordinarily, freedom is generally viewed as an unequivocally positive concept. The history of Western civilization is punctuated by a yearning and striving toward freedom. Yet, as Irvin Yalom has pointed out, freedom in the existential frame of reference can be frightening too. It means that, contrary to everyday experience, the human being does not enter and ultimately exit from a structured universe with a coherent grand design or pattern which human beings inherently find comforting and reassuring.
Freedom gives human being the responsibility for being the author of his/her own world, own life design, and own choices and actions. In one sense, the human being, as Jean-Paul Sartre puts it, is “condemned to freedom.”[52] Rollo May holds that freedom, in order to be authentic, requires the individual to confront the limits of his/her destiny.[53] If it is true, according to Jean-Paul Sartre, that we create our own selves and our own world,[54] then it also means that there is no ground beneath us: there is only an abyss, a void, nothingness.
Jean-Paul Sartre contends that humankind can freely choose or create one’s own meaning of life. However, Viktor Frankl disagrees. He points out that to ascribe to the self such a creative power would seem to be still within the old tradition of Idealism which Jean-Paul Sartre opposes. Viktor Frankl likens this freedom proposed by Jean-Paul Sartre to the fakir trick. The fakir claims to throw a rope into the air, into an empty space, and claims a boy will climb up the rope. This claim does not seem to be any different from Jean-Paul Sartre’s proposition that he tries to make us believe, Viktor Frankl contends. As a result of creating one’s own meaning of life, “man ‘projects’ himself – throws himself forward and upward – into nothingness.” [55]
One implication of this freedom and groundlessness is responsibility.Individuals differ enormously in the degree of accepting or denying responsibility for their life situations. For example, some individuals displace responsibility for their situation onto other people, onto life circumstances, onto bosses and spouses, and, when they enter counseling, they transfer responsibility for their recovery to their counselors. Other individuals deny responsibility by experiencing themselves as “innocent victims” who suffer from external events (and remain unaware that they themselves have set these events into motion).
The second implication of freedom is the will or willfulness. We have seen how the infant grows into a child, as the first virtue – hope – inspires acts of will, which is the second virtue after hope. The growing child will come to establish this will as a basic quality of character, such that some children have stronger will than others. This will allows us to act, and translates freedom and responsibility to action for better or for worse.
Rollo May points out that our will consists of two components: (1) wishing; and (2) deciding or choosing.[56] Many individuals have enormous difficulties in experiencing or expressing a wish. Wishing is closely aligned to feeling, and affect-blocked individuals cannot act spontaneously because they cannot feel and thus cannot wish. Once an individual fully experiences a wish, s/he is faced with decision or choice.Many individuals can be extremely clear about what they wish but still not be able to decide or to choose. Often they experience a decisional panic; they may attempt to avoid the whole thing altogether or to delegate the decision to someone else, or they act in such a way that the decision has been made for them by circumstances that they, unconsciously, have brought to pass and had no control. We see in the terminally ill and their family members all of these aspects. Some do not want to face reality, or even talk about their illness. Some prefer not to make any choices. Some are despondent over their inevitable destiny, and have simply given up hope, accepting fate instead.
On the other hand, there are some, perhaps fewer in number, who offer sufficient proof that everything can be taken from them but one thing: the last of the human freedoms – to choose one’s attitude in any given set of circumstances, to choose one’s own way. And there are always choices to make. Every day, every hour, offers the opportunity to make a decision, a decision which determines whether you would or would not submit to external circumstances, the powers which threaten to rob you of your very self, your inner freedom and which determine whether or not you would become the plaything of circumstances, renouncing freedom and dignity to become a victim of fate.
Hopefulness Resting in Faith. We have seen how hope can originate from the mutually trusting relationship between the infant and the mothering person. An infant’s first hope is grounded on the mothering person, who is the first verifier of the infant’s hope. One of Paul Pruyser’s major contributions is his application of Donald Winnicott’s notion of the “transitional sphere” to faith and religion.[57] Donald Winnicott has noticed that infants tend to become strongly attached to a piece of their blanket, a soft toy, a rag doll, or some other special object that they keep close to their bodies, often near their mouths. Sometimes they suck a finger while the rest of the hand holds the special object. Such action often occurs before the infant falls asleep (in the transitional stage between waking and sleeping) or when frustrated, fidgety, anxious, or depressed. Donald Winnicott called these “transitional objects” because they combine “many fragmentary elements of the total mothering situation,” yet, at the same time, help the infant to come to terms with the fact that this exclusive relationship between the mothering person and him/herself is being replaced by new experiences in which this mothering person is no longer the primary mediator of encounters with the objective world. The transitional object helps the infant make the transition from the exclusivity of the mother-infant relationship to a direct engagement with the world around him/her.[58]
In relating the transitional object to the origin of religion, Paul Pruyser suggests that the transitional object is invested with a sacred aura. It is also the focus of family rituals as other members of the family accept the infant’s view that the object of faith is special and has unique powers.[59] They treat the object with uncommon respect and caution, mindful of the righteous indignation they may provoke in the infant if they fail to reverence the object.
Paul Pruyser does not claim that transitional objects are symbols of hope, but he implies some relationship between the two when he notes that the transitional sphere may remain undeveloped, either because of the “overactivity of the inner world of dreams and hallucinatory wish fulfillment” or because one has “been goaded to notice only the outer perceptual world with its facilities and its inherent laws.”[60] Thus, those in whom the transitional sphere remains well developed are neither captive to wishful fantasy nor controlled by the world of immutable facts. As hope falls between these two extremes – that is, being more reality-testing than wishing but at the same time viewing reality as a sphere not of immutable but of ever-changeable facts – it is reflective of a well-developed transitional sphere.
Paul Pruyser notes that the transitional object assuages the infant’s anxieties and fears. William Meissner further suggests that the transitional object can be replaced by symbols (such as play or music) or rituals (such as “rites of passage”), as the infant relinquishes the transitional object for images of hope, which enable the infant to feel that he is not alone.[61] One thinks here of the enormously popular image of hope in Psalms, “Yea, though I walk through the valley of the shadow of death, I will fear no evil: for thou art with me; thy rod and thy staff they comfort me” (Ps. 23:4 AV). Many of the images employed in the book of Psalms concern the experience of transition: one walks through the valley of the shadow of death (Psalm 23); one is drawn up from the miry bog (Psalm 40); one is like a leaning wall or a tottering fence, about to be brought down (Psalm 62); and one is like grass that flourishes in the morning and fades and withers by evening (Psalm 90). In the Psalms, we live between the times, and we experience God in the process of moving from one secure point to another. As Psalm 121 has it: “The LORD shall preserve thee from all evil: he shall preserve thy soul. The LORD shall preserve thy going out and thy coming in from this time forth, and even for evermore” (Ps. 121: 7-8 AV)
It is no accident, then, that the God who is addressed in the psalms is preeminently identified with hope. Nor it is surprising that, in many of the psalms, emotions reflective of the three stages of wishing are often intermingled with feelings reflecting hope: the paranoia of the waiting stage, the obsession of the anticipation stage, and the masochism of the pining stage. Yet, these only make the psalms’ convictions of hope all the more impressive, as hope is the predominant theme of each psalm and of the psalms as a whole.[62]
It is also not surprising that the transition from our present life to the life that awaits us after death is most effectively portrayed through music. As the book of Revelation has it: “And I heard a voice from heaven, as the voice of many waters, and as the voice of a great thunder: and I heard the voice of harpers harping with their harps: and they sung as it were a new song…” (Rev. 14:2-3 AV). Thus, music has a unique association with hoping. We know this, of course, from the fact that groups and movements that hope for a better tomorrow are often sustained in their hope by shared songs of faith and the ritual of communal singing (“We Shall Overcome”). Conversely, hopelessness is often experienced as soundless-ness, or, at best, the almost inaudible sounds of low moaning with which we associate the pining of unrequited love and inexpressible grief.
Death and Hopefulness
Among all the existential concerns,death is the most obvious one. It is apparent to all that death will come to every one of us, and that there is no escape. It is a terrible truth, and at the deepest levels we respond to it with mortal terror, because as Baruch Spinoza states, everything wishes to “persist indefinitely in its own being.” [63] From the existential point of view, there is a core inner conflict between our awareness of inevitable death and our simultaneous wish to continue to live.
Most of us have the desire that death will not be final, and that whatever form our existence may take after we die, it will be more whole and complete than our earthly life has been. What images of life beyond the grave typically do for us is to enable us to envision the reversal of the ultimate loss resulting from personal death. We have this desire, but we differ a great deal in our anticipation that this will in fact occur. For some of us, our anticipation of such an afterlife is very strong. For others, it is rather weak. Its strength or weakness is influenced by many factors but is related in part to whether we have found a way to image our future beyond the grave.
Some of the terminally ill do not want to face the reality of death. Perhaps that was why Mr. Zhang did not ask about the seriousness of his illness.[64] Culturally speaking, it is taboo for Chinese people to talk about death. Besides, it is widely believed by the Chinese that patients with late stage cancer may become despondent and simply give up when they are told that they have the big “C.” These patients may feel so powerless and hopeless that they no longer wish to engage in the ordinary tasks of living. Like the prisoners in the Nazi concentration camps, they may literally lie down and die, accepting their portion of fate or destiny. There are, however, others who cling to their images of hope that will sustain them when death is knocking on the door.
In his poem “Bright Star, Would I Were Steadfast as Thou Art,” John Keats describes the stars as eternal watchers over the events of earth.[65] He notes how they observe the motions of the sea, and how they watch the snow falling from their privileged vantage point far above the earth. He also pictures them watching his beloved at sleep. By projecting onto the stars the ability to watch, and to watch forever, John Keats expresses his own desire to be as the stars, to be able, like them, to gain a privileged vantage point from which to watch the scenes of earth. If only he could become an eternal watcher over the natural, recurrent events of the sea’s ebb and flow and the snow’s descent. If only he could watch his beloved, night after night, as she sleeps peacefully in quiet repose.
John Keats wrote this poem when he knew that he had a terminal illness during his medical studies. [66] He died just a few months later, at the age of twenty-six. This poem projects an image of hope: his hope that, as his earthly life draws to a close, he will be “lifted up” to take his place among the eternal watchers and will then be able to see with clarity what he now sees only in partial and distorted ways. Through this imagery, the future is more palpably real and present to him, and this image of hope is a stay against the personal despair that he found himself fighting, day after day, as death drew nigh.
Hopefulness Resting in Rational Thoughts and Actions. Genuine hope is based on what is possible for us. Based on what we know about ourselves, we may anticipate that certain things are possible for us and others are not. We weigh the possibilities that are in front of us in light of our understanding of ourselves, our temperament, our traits, our motivations, and our values. This weighing requires rational thoughts to choose goals that are realizable for our own good.
In addition, chosen goals can be redirected or re-defined through rational thought process. In the terminally ill, one’s hope appears to be centered less on the anticipation of cure than on asking other questions such as: how long one can expect to live, how painful it will be, how severe will be the physical and mental debilitation, and the extent to which the pain and debilitation can be moderated by painkilling drugs. If hope is to survive in situations where the loss is inevitable and irreversible, our hopes may need to be re-centered. This may involve focusing on other realizable goals, and calling on various resources to attain them. This requires rational actions. It is important to start taking small steps toward the bigger goal. For the terminally ill, these can also be short term goals, such as surviving at least through the Christmas season, or getting one’s financial affairs in order, or becoming reconciled with a particular family member, or resolving not to succumb to personal bitterness but to maintain one’s good humor to the end.
During this process of calling forth rational thoughts and actions, the hopeful person needs a certain sense of control; without it, feelings of powerlessness or hopelessness would set in. We see this even in infants as they demonstrate trust in self and in the world as an early form of control in the development of hopefulness. They struggle to control their hostile urges toward the mothering person so as not to cause this person to withdraw from them: “For the growth of autonomy, a firmly developed early trust is necessary. The infant must have come to be sure that her/his trust in both self and the world will not be jeopardized by the violent wish to have one’s own choice. As the child learns to exercise self-control over her/his own willfulness, autonomy emerges. As one’s sphere of activity expands, hopes are no longer limited to expectations of the mothering person. The whole world becomes one’s verifier of hope. The young child learns to change the world by choosing goals and deciding to move forward to fulfill them. This helps the young child to transcend above present circumstances and set her/his sight to the future. By exercising such a capacity, the young child defines her/his identity, gives meaning and coherence to her/his life, and takes responsibility for the kind of person s/he is.”[67] This responsibility lasts a life time as the child grows, just as Viktor Frankl states, “Life ultimately means taking the responsibility to find the right answer to its problems and to fulfill the tasks which it constantly sets for each individual.” [68] In conclusion, the author believes that fostering hope in the terminally ill is justified in dealing with their existential concerns.
Research Consideration
Using the Beck Hopelessness Scale, Elizabeth Rideout and Maureen Montemuro found that “patients who are more hopeful maintain their involvement in life regardless of physical limitations imposed by their heart failure.”[69] They were not necessarily better by functional measures, nor did they live longer, but they maintained their “involvement in life.” Hope seems to be life-giving in this sense, but it is hard to know from this study whether “involvement in life” gives hope or whether hope gives “involvement in life.” Another study in Canada (1994) with cardiac patients waiting for heart transplant suggested that “hope was the only variable that contributed to coping.” [70] These two studies, when taken together, point in the direction that hope helps persons with heart failure to maintain their involvement in life, and persons awaiting heart transplant to cope with the waiting period.[71] Hope can help us to live until we die, or until we receive a second chance at life.
Joni Eareckson Tada, who has been a quadriplegic for almost thirty years as a result of a traffic accident, has influenced countless others with her writings and speaking engagements. She stated that her ability to minister to others in pain and suffering provided meaning in her own life: “The longer I hung in there through the process of suffering, the stronger the weave in the fabric of meaning.”[72] She and countless others have demonstrated that there can be quality of life even in the most trying of circumstances. For them, the values and meaning of life depend not so much on good health as a positive attitude towards life.
Doris Coward reported that patients with Acquired Immune Deficiency Syndrome (AIDS) found meaning and purpose through reaching out, having hope, connecting with others, and having a purpose to fulfill. [73] Betsy Fife found that the meaning people attribute to having cancer affects how they copewith this disease. [74] Miriam Cameron interviewed a number of patients with AIDS and their significant others. [75] She provided numerous accounts that suggest that people can live with dignity in spite of chronic conditions and terminal illness, if they have faith, hope and a sense of meaning and purpose. One of the conclusions Miriam Cameron drew from her interviews was that, in general, health care personnel are poorly prepared to help these patients and their loved ones to deal with ethical and existential issues of death. There is indeed an urgent need for compassionate and competent providers of pastoral care and counseling.[76]
There is also increasing evidence that proper palliative care can enable patients to live and die with dignity. For example, Mary Jane Massie et al.[77] found that in cancer patients, depression, a sense of hopelessness, feelings of loss of control, poorly controlled pain, limited family and social support, and cancer treatment, rather than the cancer itself, contributed to one’s desire to end one’s life. Pain control, antidepressant medication, support, and psychotherapyalleviated their suicidal feelings and enabled them to go on to live with their illness.
Douglas Smith and Michael Maher[78] studied hospice coordinators who reported that dying individuals who experienced “good death” tend to have the following qualities: having a sense of control, discussing the practical implications of dying, exploring an afterlife, talking about religious/spiritual issues, reviewing the past, having a sense of humor, not avoiding painful truths, taking an interest in personal appearance, the presence of significant others, and participating in physical expressions of caring.
Stewart Alsop’s memoirs provided an inspiring case study. After he was told that he had an inoperable and lethal cancer, acute myeloblastic leukemia, Stewart Alsop wrote about his past, including his thoughts about suicide while waiting for another marrow test in the hospital room. But after the first bad night, having been told of the imminence of his death, a kind of protective mechanism took over. Even though he was not a religious person, he believed that “there is certainly a mystery out there somewhere. In a way, we are all religious whether we like it nor not…Even if my stay of execution turns out to be a short one, I have reason to be grateful, for a happy marriage and a reasonably long, amusing, and interesting life.” [79] Throughout the ups and downs of his illness, he grew to appreciate life and embrace death.
In another case study, Thomas Cole discussed the insights he gained from reading Claire Philip’s journal entries. After learning she was struck with cancer, Claire Philip, a clinical social worker, turned to journal writing to communicate her feelings and inner struggles. In her June 15, 1991 entry, she writes: “I see that I am weeping for the waste of my own potential, too, and for the loneliness of nearly silent years in which I struggled to manage being ill…” The last pages of her journal indicate an acceptance of death as well as a continued engagement with life. In spite of her weakened physical condition and lingering fevers, she still had “a few hours of creative time each day.” In her last entry, even when life was ebbing away, her love for life was still evident:
“I started a book I find light enough to enjoy, and I am writing, and the newsletter piece on ethics and life-threatening illness just came out in the Ohio Clinical Reporter today. That and a visit from L.C. that ranged over a few subjects and brought a few laughs – it’s still something. Let there be something, enough every day for a while.” [80]
In spite of tremendous discomfort and pain, she proved that the human spirit can continue to grow until the very end. Thomas Cole concluded that “her journal demonstrates that it is possible to live out the paradox inherent in the proverb: Live every day as if you will be able to do good for a hundred years and live every day as if it were your last.”
Biology of Hope
Norman Cousins(1915 – 1990), an avid researcher at UCLA on the effect of positive emotions on health, narrates his experiences in his book, Head First: The Biology of Hope. He tells of a conversation overheard between two oncologists. One says, “You know, Bob, I just don’t understand it. We used the same drugs, the same dosage, the same schedule, and the same entry criteria. Yet I got a 22 percent response rate and you got a 74 percent rate. That’s unheard of for metastatic lung cancer. How do you do it?” Bob replies, “We both used Etoposide, Platinol, Oncovin, and Hydroxyurea. You call yours EPOH. I tell my patients I’m giving them HOPE. Sure, I tell them this is experimental, and we go over the long list of side effects together. But I emphasize that we have a chance. As dismal as the statistics are for non-small cell, there are always a few percent of people who do really well.” Norman Cousins says, “Don’t deny the diagnosis. Try to defy the verdict.” [81] The hard core of Norman Cousin’s book is a chapter called “Belief Becomes Biology.” In this chapter he reports on scientific studies which indicate how hope can promote healing. Norman Cousins died in 1990, but two studies which bear his name as co-researcher appeared in that year.
Cancer patients – persons with malignant melanoma – were divided into two groups. The control group received the standard medical care. The experimental group received medical care plus a six-week structured psychiatric group intervention. This intervention consisted of health education, problem-solving, stress management, and group support. The outcome was measured at two points. At the end of six weeks, experimental subjects “exhibited higher vigor and greater use of active-behavioral coping than the control.” At six-months follow up, the differences between the two groups were even more pronounced. This study concludes: “These results indicate that a short-term psychiatric group intervention for patients with malignant melanoma effectively reduces psychological distress and enhances longer-term effective coping.” [82]
A second study based on the same six-week group intervention was published in the same issue of the journal. It reported the following changes in immunological measures: “Significant increases in the percent of large granular lymphocytes and natural killer cells along with indications of increase in NK cytotoxic activity and a small decrease in the percent of T Cells.” [83] The significance of these immunological results is not clear, and to my knowledge, there have been no follow up studies. However, these two studies suggest that brief group therapy, focusing on skills and support, can reduce psychological distress, enhance effective coping, and increase certain immunological measures.
An even more striking study on the impact of group intervention was reported by David Spiegel et al. in 1989 Lancet, a highly reputable British medical journal.[84] The authors studied the effect of psychosocial treatment on survival of patients with metastatic breast cancer. The intervention in this study was one year of weekly supportive group therapy. Patients were followed not just for six months, but for ten years. Women in the treatment group survived twice as long (36.6 months) as women in the control group (18.9 months). What is more, three women were still alive at the end of this ten-year period, and they were all in the treatment group. These are astounding results, all the more so because the researchers say, “We expected to improve the quality of life without affecting its quantity.” The validity of this research was confirmed in 1997 journal Cancer.[85] Taken together, these studies indicate that not only can group therapy relieve psychological distress, improve coping, and increase immunity, it can lengthen survival.
Nothing is said specifically about hope in Norman Cousins’ studies or this one. One would have to assume that hope was a component of the group therapy. That is not an unreasonable assumption. Irvin Yalom lists ten therapeutic factors in group therapy. [86] The first of these is “the instillation of hope” and the last is “existential factors” such as meaning and purpose. It is not a big leap to bring in Irvin Yalom, because Irvin Yalom was a co-researcher with David Spiegel in an earlier study on group therapy with the dying.[87] And David Spiegel’s description of the type of therapy in the present study says, “Patients focused on how to extract meaning from tragedy by using their experience to help other patients and their families.”
Finally, a 1996 report [88] suggested that “hopelessness is a strong predictor of adverse health outcomes, independent of depression and traditional risk factors.” Specifically, men with a high degree of hopelessness were three times as likely as those with low hopelessness to die in the six-year period. If you are unhealthy, your chance of dying in the next six years is three times as great, without hope. If you are healthy, it is six times as great. Literally, without hope, we die.
In conclusion, there is a wealth of
literature to justify the ethics, the application and potential benefits of
fostering hope in the terminally ill. The next chapter deals with how this
fostering can be done, with consideration given to the cultural context in
China.
[1] In this dissertation, fostering hope means promotion of growth or development of hope. It is used here to include both the inspiration and nurturing of hope.
[2] James Greek, cited in Spirituality, Health, and Wholeness: An Introductory Guide for Health Care Professionals, ed. Siroj Sorajjakool and Henry Lamberton (New York: Haworth Press, 2004), 110.
[3] Charles A. Corr, Clyde Nabe and Donna Corr, Death and Dying, Life and Living, 4th ed. (Belmont, CA: Wadsworth, 2003), 140.
[4] Elizabeth Kübler-Ross, On Death and Dying (New York: Macmillan, 1969), 99.
[5] Corr, Nabe and Corr, Death and Dying, Life and Living, 139.
[6] Paul T. P. Wong, “The Wisdom of Positive Acceptance,” President’s Column, International Network on Personal Meaning (2004), http://www.meaning.ca (accessed May 14, 2008).
[7] Frankl, Man’s Search for Meaning, 75.
[8] Lao-tzu, Tao Te Ching, Book 1, chap. 8, 64.
[9] Encyclopedia Britannica, “Daoism,” http://www.britannica.com/EBchecked/topic/582972/Daoism (accessed May 14, 2008).
[10] Interview #23, Appendix.
[11] Merle H. Mishel, “The Theory of Uncertainty in Illness,” Image 20, no. 4 (1988): 229.
[12] Ibid., 231.
[13] Interview #10, Appendix.
[14] Avery D. Weisman, On Dying and Denying: A Psychiatric Study of Terminality (New York: Behavioral Publications, 1972), 67-74.
[15] Richard S. Lazarus, “Positive Denial: The Case for Not Facing Reality,” interviewed by Daniel Goleman in Psychology Today 48 (November 1979): 44.
[16] Richard S. Lazarus, “Stress and Coping as Factors in Health and Illness,” in Psychosocial Aspects of Cancer, ed. Jerome Cohen et al (New York: Raven Press, 1982), 175.
[17] Inge B. Corless, “Hospice and Hope: An Incompatible Duo?” American Journal of Hospice and Palliative Care 9 (May/June 1992): 10.
[18] Yalom, Existential Psychotherapy, 8.
[19] James E. Loder, The Transforming Moment: Understanding Convictional Experiences (San Francisco:
Harper & Row, 1981), 79-91.
[20] Andrew D. Lester, Hope in Pastoral Care and Counseling, chap. 5, 80.
[21] Loder, Transforming Moment, 167-73.
[22] Frankl, Man’s Search for Meaning, 115.
[23] Debra Parker-Oliver, “Redefining Hope for the Terminally Ill,” American Journal of Hospice and Palliative Care 19, no. 2 (2002): 115.
[24] Deborah R Mitchell, “The ‘Good’ Death: Three Promises to Make at the Bedside,” Geriatrics 52, no. 8
(1997): 591-92.
[25] Parker-Oliver, “Redefining Hope for the Terminally Ill,” 115.
[26] Elizabeth Kübler-Ross, “Therapy with the Terminally Ill,” Death: Current Perspectives, ed. Edwin S. Shneidman, 2nd ed. (Palo Alto, CA: Mayfield Publishing, 1980), 201.
[27] Parker-Oliver, “Redefining Hope for the Terminally Ill,” 115.
[28] Cathleen Fanslow-Brunjes, Patricia E. Schneider, and Lee H. Kimmel, “Hope: Offering Comfort and Support for Dying Patients,” Nursing 27, no. 3 (1997): 54-57.
[29] John MacMurray, Persons in Relation (London: Faber & Faber, 1961), 150.
[30] Martin Buber, I and Thou, trans. Walter Kaufman (Edinburgh: T. & T. Clark, 1970-1), 62.
[31] Story of Ms. Zeng in Chapter 2, page 54. Interview #12, Appendix.
[32] Sigmund Freud, “Inhibitions, Symptoms and Anxiety,” Standard Edition of the Complete Psychological Works of Sigmund Freud, vol. 20 (London: Hogarth Press, 1959), 119-23.
[33] Yalom, Existential Psychotherapy, 353.
[34] Ibid., 23 on transcendental self.
[35] Ben Mijuskovic, Loneliness in Philosophy, Psychology, and Literature (Assen, Netherlands: Van
Gorcum, 1979), 99-100.
[36] Walter Brueggemann, Hope within History (Atlanta: John Knox Press, 1987), 84.
[37] Elaine Scarry, The Body in Pain: The Making and Unmaking of the World (New York: Oxford
University Press, 1985), 34.
[38] Stanley Hauerwas, Naming the Silences: God, Medicine, and the Problem of Suffering (Grand
Rapids, MI: Eerdmans Publ., 1990), 146.
[39] Ibid.
[40] Story of Mr. Zhang in Chapter 3, page 71. Interview #8, Appendix.
[41] Anderson, Spiritual Care-giving as Secular Sacrament, 58.
[42] Pruyser, Between Belief and Unbelief, 187.
[43] Pruyser, Between Belief and Unbelief, 187.
[44] Lee E. Snook, “Death and Hope – An Essay in Process Theology,” Dialog 15, no. 2 (Spring 1976): 127.
[45] Hauerwas, Naming the Silences 146.
[46] Robert Beavers and Florence Kaslow, “Anatomy of Hope,” Journal of Marital and Family Therapy 7, no. 2 (April 1981): 125.
[47] Carrigan, “Where Has Hope Gone?” 39.
[48] William F. Lynch, Images of Hope: Imagination as Healer of the Hopeless (Baltimore: Helicon, 1965), 19.
[49] Gabriel Marcel, “Despair and the Object of Hope,” The Sources of Hope, trans. Joan Notwotny, ed. Ross Fitzgerald (Rushcutters Bay, Australia; Elmsford, NY: Pergamon Press, 1979), 47.
[50] Lynch, Images of Hope, 136-37.
[51] Ibid., 219.
[52] Jean-Paul Sartre, Being and Nothingness: An Essay in Phenomenological Ontology, trans. Hazel E. Barnes (New York: Citadel Press, 1956), 631.
[53] Rollo May, Freedom and Destiny (New York: W. W. Norton, 1981), 93-96.
[54] Sartre, Being and Nothingness, 631.
[55] Viktor Frankl, The Unconscious God (New York: Simon and Schuster, 1975), 58.
[56] Rollo May, Love and Will (New York: W. W. Norton, 1969), 218.
[57] Donald W. Winnicott, “Transitional Objects and Transitional Phenomena” in Collected Papers: Through Paediatrics to Psycho-Analysis (New York: Basic Books, 1958), 229-42.
[58] Pruyser, Play of the Imagination, 110-11.
[59] Pruyser, Between Belief and Unbelief, 198-213.
[60] Ibid., 114.
[61] William W. Meissner, Psychoanalysis and Religious Experience (New Haven: Yale University Press, 1984), 169.
[62] Donald Capps, Biblical Approaches to Pastoral Counseling (Philadelphia: Westminster Press, 1981), 206-8.
[63] Baruch Spinoza, cited in The Tragic Sense of Life by Miguel de Unamuno, trans. J. E. Crawford Flitch (New York: Cosimo Classics, 2005), 22. Publication information for Baruch Spinoza not provided.
[64] Mr. Zhang’s story from Interview #8, Appendix.
[65] John Keats, “Last Sonnet,” in The Poetical Works of John Keats, ed. H. Buxton Forman (London: Oxford University Press, 1931), 486.
[66] Capps, Agents of Hope, 65, as he quoted the work of Aileen Ward in John Keats: The Making of a Poet (New York: Viking Press, 1963), 297-300.
[67] Gerald Dworkin, The Theory and Practice of Autonomy (New York: Cambridge University Press, 1988), 20.
[68] Frankl, Man’s Search for Meaning, 85.
[69] Elizabeth Rideout and Maureen Montemuro, “Hope, Morale and Adaptation in Patients with Chronic Heart Failure,” Journal of Advanced Nursing 11 (1986): 429-38.
[70] Alexandra M. Hirth and Miriam J. Stewart, “Hope and Social Support as Coping Resources for Adults Waiting for Cardiac Transplantation,” Canadian Journal of Nursing Research 26, no. 3 (1994): 31-48.
[71] Interview #14, Appendix.
[72] Joni E. Tada, When Is It Right to Die? Suicide, Euthanasia, Suffering, Mercy (Grand Rapids, MI: Zondervan Publishing House 1992), 85.
[73] Doris D. Coward, “Meaning and Purpose in the Lives of Persons with AIDS,” Public Health Nursing 11 (1994): 331-36.
[74] Betsy L. Fife, “The Measurement of Meaning in Illness,” Social Science Medicine 40 (1995): 1021-28.
[75] Miriam E. Cameron, “Technical Problems Involving Death,” AIDS Patient Care: A Journal for Health Care Professionals 8 (October 1994): 269-78.
[76] Paul T. P. Wong and Catherine Stiller, “Living with Dignity and Palliative Care,” in End of Life Issues: Interdisciplinary and Multidimensional Perspectives, ed. Brian de Vries (New York: Springer, 1999), 77-94.
[77] Mary Jane Massie et al., “Depression and Suicide in Patients with Cancer,” Journal of Pain and Symptom Management 9 (1994): 325-340.
[78] Douglas C. Smith and Michael F. Maher, “Achieving a Healthy Death: The Dying Person’s Attitudinal Contributions,” Hospice Journal 9 (1993): 21-32.
[79] Stewart Alsop, Stay of Execution: A Sort of Memoir (New York: J. B. Lippincott, 1973), 150.
[80] Thomas R. Cole, “Gaining and Losing a Friend I Never Knew: Reading Claire Philip’s Journal and Poetry,” Journal of Aging Studies 9, no. 4 (Winter 1995): 329-34.
[81] Cousins, Head First: The Biology of Hope, 34, 79.
[82] Fawzy I. Fawzy, Norman Cousins, et al., “A Structured Psychiatric Intervention for Cancer Patients. I. Changes over Time in Methods of Coping and Affective Disturbance,” Archives of General Psychiatry 47, no. 8 (1990): 720-25.
[83] Ibid., 729-35.
[84] David Spiegel et al., “The Effect of Psychosocial Intervention on Survival of Patients with Metastatic Breast Cancer,” Lancet 2 (Oct. 14, 1989): 888-91.
[85] Manuela M. Kogon, David Spiegel et al., “Effects of Medical and Psychotherapeutic Treatment on the Survival of Women with Metastatic Breast Carcinoma,” Cancer 80, no. 2 (July 15, 1997): 225-30.
[86] Irvin D. Yalom, The Theory and Practice of Group Psychotherapy, 4th ed. (New York: Basic Books, 1995), 3-4.
[87] David Spiegel and Irvin D. Yalom, “A Support Group for Dying Patients,” International Journal of Group Psychotherapy 28, no. 2 (1978): 233-45.
[88] Susan A Everson-Rose, George A Kaplan, Johanna Salonen and Debbie E. Goldberg, “Hopelessness and Risk of Mortality and Incidence of Myocardial Infarction and Cancer,” Psychosomatic Medicine 58, no.2 (March 1996):113-21. ·
CHAPTER 6: Fostering Hope in the Terminally Ill
General Considerations
Hope can be fostered in the terminally ill through a number of ways, based on our understanding of the four dimensions of hope: through the creation or discovery of meaning in their lives; through a trusting relationship of love and support in which hope can be inspired and nurtured; through spiritual empowerment; and through goal-setting and goal-achievement.
Through Creation or Discovery of Meaning
Personal Narratives. Every person has a narrative to tell. A narrative is a story: an interpretation of some aspect of the world that is historically and culturally grounded and shaped by human personality.[1] In another sense, a narrative is a structure by which we construct our experiences of others as well as of ourselves. In these narratives, we create our own meanings.[2] A quote from Sartre says, “Humans are always tellers of tales; we live, surrounded by our stories and the stories of others. We see everything that happens to us through these stories; and we try to live our lives as if we were telling a story.” [3] Revealing our stories is the only effective way to communicate our sense of self to another person. It is imperative to know a person’s full narrative, including its full temporal dimensions, when trying to make sense of this person’s life situation and relate this person’s meaning to hope.[4]
As we encounter the world, each new sensation, stimulus, and interpersonal event is shaped by our mental processes into a story, according to some meaningful organizing principles (guiding metaphors) called narrative structures.[5] An event accrues meaning only as we apply narrative structure that connects the event to its impact on the future – the consequences for the rest of the story. Stephen Crites was one of the first to conceptualize that human life occurs in narrative form.[6] Human beings do not simply tell stories, or illustrate their lives with storytelling. We construct our sense of identity out of stories, both conscious stories and those we suppress.
A core narrative is the central interpretive theme that provides an individual or system with an overarching structure that organizes and makes sense out of a particular aspect of the human condition. It is composed of numerous smaller stories. Individuals have core narratives that structure their understandings and values around concepts such as suffering, life and death. For example, religious faith can supply core narratives that explain these concepts as well as prayer and meditation. Our experiences, then, are given their individual distinctiveness, their form as our story, through the structure of narrative.[7] Our sense of self, our identity, is built piece by piece as we form our experiences into stories and then integrate these stories into our ongoing core narratives. The core narratives of a person’s life, rather than mere data about that person, set the parameters of that individual’s sense of self. Simply referring to facts about a person does not really allow us to know that person. Hannah Arendt says that we cannot effectively answer the question – Who is she? – by describing the “what” about her (such as a description of her physical attributes, facts about vocation, or information about organizational memberships), because in presenting such lists of characteristics, the person’s uniqueness escapes us.[8] The question – Who is she? – can be answered only by referring to the whole “story” of that individual. We do not sense that we really know someone until we begin to hear that person’s story and identify the core narratives. The core narratives communicate a person’s values, purposes, unique characteristics and experiences which allow us to imagine an identity from which we begin to experience that person and form our own story about that person.
This narrative theory, together with Erik Erikson’s developmental theory, provides the rationale for the reminiscence approach to promoting the psychological health of an individual.[9] In his developmental theory, Erik Erikson describes a person’s last developmental task as the reworking of one’s past, culminating in either ego integrity or despair (hopelessness).[10] The maintenance of ego integrity – that is, the acceptance of one’s life (failures and all) and the holding up of confidence – is essential to hopefulness. Erik Erikson’s apt phrase is, “to be – through having been.” [11] Not uncommonly, the terminally ill would get a respite from the present pain and suffering while reminiscing past achievements with pride. Other gains may include reconciliation of relationships, acceptance of mortality, and contentment in having done one’s best.[12] The caregiver’s supportive listening and promotion of self-expression will help to restore a sense of personal meaning, identity, and role in the cared-for. Photographs, memorabilia, music and what-not can be used to recall memories of childhood events, celebrations, etc. Interventions should be minimal and timed only according to cues from the cared-for. Confidentiality should be respected. [13]
Through life reviews that help to re-integrate unresolved conflicts, Robert Butler has had some success with treating depressed patients through processes of reconciliation and acceptance of mortality, as well as instilling pride in accomplishment and a feeling of having done one’s best.[14] Gerontologist Peter Coleman also found that the teaching function of informative reminiscence (that is, passing on of knowledge or attitudes) mostly benefits those facing severe role loss in old age.[15] By reaffirming a sense of identity, uniqueness, self-worth and accomplishment, reminiscence can assist patients in their adaptation to multiple losses and their maintenance of self-esteem. He also reported that “the consoling use of the past would occur more often in the presence of considerably changed circumstances threatening (one’s) sense of self-continuity.”[16] Asking the patients to talk about what has given meaning in the past can also help them verbalize feelings that lead to meanings in the present situation.
Reframing Hope. Using past goals, achievements, or even frustrations to find new opportunities and possibilities in the future is one way to reframe meaning and hope for the present.Frames are the ways we perceive events of circumstances; they shape our reality. Reframing changes those perceptions. It constructs for people a new way to organize and view their experiences and turns liabilities into strengths. For example, more than once I heard patients say that their illnesses had brought the family closer. Instead of framing hopelessness, they were reframing their hope on the unity and harmony of the family. Similarly, instead of framing their hope on having their illnesses cured, they are reframing their hope on peace and comfort. As meanings change, individuals react to similar situations with very different feelings, thoughts, attitudes, and behaviors.
The reframing method comes from neuro-linguistic programming [17] and family therapy theory.[18] To reframe is to reshape perceptions, to change the cognitive sets by which individuals, families, or groups interpret events or relationships, to transform the way in which they conceptualize a life situation. Once they entertain even the slightest doubt about any portion of their frame – once they consider that there may be another way of looking at events – they find it hard to return to their previous point of view. [19] They begin to visualize a future without the problem.
Reframing helps people to rearrange the furniture and change the decorations in a certain room of their memory – that is, change their understanding of the past. Reframing also encourages people to develop a new perception of their present situation and to reshape their ideas about the future. When they reveal to the one-caring a negative frame composed of images that contradict hope, shifting to a positive frame will help them envision a hopeful future.
Certain events are more difficult than others to frame positively. They may appear to offer little that is good. For example, when Mr. Li had run out of money, and could not afford even pain relief, there was really little to frame positively.[20] Asking him why he did not kill himself brought out his reasons for living, reasons that only he would have known for sure. When some people find it really hard to think of anything positive in their situation, it is still vital to let in some positive information, even if one has to work hard at believing it. Andrew Lester suggests “urging those who have difficulty believing any positive frame to act temporarily as if the reframed way of viewing a situation is true. Strike a deal with them, if necessary, or ask them to humor you. If they object that it would be hypocritical, agree with them; propose that they be a ‘hypocrite for a day’ (or longer).” [21] If in doing so they experience any positive change in feelings or behavior, encourage them to continue acting as if the frame is true.
Help the cared-for recall past situations in which they had solved a problem, or even ways in which they were addressing some present difficulty. The one-caring can promote different perspectives, helping the cared-for to reframe what is happening so that hope grows and positive change appears possible.
Telling Future Stories. Another way to foster hope in the cared-for is to invite them to identify or create stories about specific future events. Using the imagination to spin a tale gives particularity to what was previously unspeakable. Narrative theory demonstrates the power of stories for affecting the way in which people construct their worldview. [22] Using future story-telling, the one-caring can invite the cared-for to imagine a future that is hopeful, to reach for positive values, to experience a joyful life. For example, start with questions such as: [23]
If your life was made into a movie with a happy ending, tell me what the ending of the movie would look like.
If you wrote me a letter in a few years and it was filled with good news about your life, what would the letter say?
If I read a story in the newspaper next year about something wonderful that happens to you, what would it be?
Next ask them to add details – people, places, scenes, and events – until they describe a fairly clear and concrete future story that could serve as a basis for choosing creative behaviors and adopting a more hopeful stance toward the future.
Richard Gardner’s mutual storytelling method can help people form more hopeful future stories. Richard Gardner, a child psychiatrist, invites children to tell stories for his “Make-Up-A-Story Television Program,” [24] informing them that he, too, will be telling stories. He instructs them to make up a story that has a beginning, a middle, and an end. After they finish the story, Richard Gardner asks them to tell what the story means. He decides what part of the story needs to be challenged in order to provide an alternative frame of reference and then, using the same characters and story line, retells the story with a different outcome. Pastoral caregivers can adapt Richard Gardner’s guidelines for retelling adult stories made up by the cared-for about the future. In particular, the pastoral caregivers can look for places where a liability can turn into an asset, a disappointment into an opportunity, a crisis into a chance for growth, thus leading to a positive or hopeful dénouement.
Guided Imagery. Guided imagery takes advantage of the human capacity for imagination and the ability to project pictures in the mind’s eye.[25] It can help people discover their own future stories and also reframe, or reconstruct, a new future story. The cared-for first close their eyes and establish a calm, meditative attitude. Once they are relaxed, ask them to choose a time frame and form a mental picture while describing future possibilities. Next, lead them through various images or fantasies that suggest creative new ways of seeing the time to come, and explore together further ideas for alternative futures.[26] Many people find that this exercise facilitates their efforts to project into the future; the resulting narrative will reveal their own visions of the future. The poem “Bright Star, Would I Were Steadfast as Thou Art” written by John Keats is one image of hope that is a stay against the personal despair he found himself fighting, day after day, as death drew nigh.[27]
When the cared-for succeed in discovering or creating new meaning, there can be a sense of control over the chaos and vulnerability of life. When the framing on suffering and death is reframed to redemption and life, then hope emerges in the far horizon.
Through a Relationship of Love and Support
Parker-Oliver suggests that keeping an inventory of key relationships can provide opportunities to establish meaning and purpose. Understanding and evaluating them can lead patients to new goals and hopes, one of which is reconciliation.[28] Ira Byock suggests that there are five things that can be said to repair broken relationships. Those things include: “Forgive me,” “I forgive you,” “Thank you,” “I love you” and “good-bye.”[29] Exploring opportunities to rebuild or enhance mutually trusting relationships gives life essential meaning. On the other hand, terminating non-mutual relationships may be necessary because they foster despair rather than hope.
The caregiver’s relationship with the terminally ill is critical in fostering hope. Hope can be discovered in a mutuality of trust and care, established through empathic listening and reflections; through compassion, respect, and acceptance; through one’s presence; and through one’s unwavering commitment in providing care and comfort. New or rediscovered friendship can open up the future and produce energizing hope. Having a friend who cares will provide the vehicle of hoping and sharing one’s ecstasies and disappointments. “The friend who can be silent with us in a moment of despair or confusion, who can stay with us in an hour of grief and bereavement, who can tolerate not-knowing, not-curing, not-healing and face with us the reality of our powerlessness, that is the friend who cares.” [30]
Through Spiritual Empowerment
Assessment of an individual’s spirituality provides yet another opportunity for exploring the possibility of hope. Spirituality offers the hope of transcendence through devotional reading, prayers and meditations, music and songs, legacies and traditions to honor memories, and rituals to facilitate spiritual relief and release from burden or guilt. Many belief systems hold out the hopes of happiness and peace for their believers. A promise of life after death is an important one. This afterlife can take many forms. Even without an alignment with religious dogma, doctrine, or creed, a dying person will usually enter a spiritual journey in a quest for meaning during this unique phase of life. Spiritual issues have been found to be the most common topic of discussion in hospice patients. [31] Discussions of such matters, in fact, tie the living to the dying, and the dying to those who have died before them. The search for peace and harmony in the last days does open up many opportunities for hoping. In addition, serving others often will benefit the terminally ill as they find their experiences meaningful and spiritually uplifting.
Imagine a Miracle. Another way of getting spiritual empowerment is through imagination. Throughout time, human beings have fantasized about changing their lives with the wave of a wand, a magic word, a stroke of good luck, or a miracle. Steve de Shazer et al. have taken advantage of this human desire and used it for therapeutic purposes. They employ what they call the miracle question to spark images about the future: [32] “Suppose you wake tomorrow morning and your problem is miraculously gone. How would you know? How would you recognize the change? How would your family or friends know? What would be different in your life? ”
Ben Furman and Tapani Ahola ask the cared-for to imagine a time in the future when their problem no longer exists.[33] They start with questions such as “How is your life these days?” “Tell me about your problem.” Then they encourage the cared-for to talk about that imaginary future time when the problem magically disappears. They ask “What would you imagine your life would be like then?” “What would be some of the significant changes in your life?” Usually, the cared-for are able to describe what would have changed in themselves and others in order for the imagined future to occur. The seeds of change lie within those descriptions. They use the descriptions given by the cared-for to guide interventions and shape revised future stories. They point out that imagining a miracle can transport people beyond their despairing images of the future. For those who contemplate suicide, pastoral caregivers may raise the future issue by asking them to imagine that, having died, they are met at heaven’s gate by an angel who announces a reprieve and sends them back to earth with all their problems solved:[34] “What will life be like for you with your problem solved and a chance to start over?” Working with those possibilities, the cared-for can begin to construct a future that is workable in the present.
Through Goal-setting and Goal-achievement
While hope can be fostered by encouraging the cared-for to envision a new future, it can also be fostered by helping them to develop specific objectives that can move them toward that future. Establishing goals is a critical but sometimes difficult task because so many people seem frozen in the unchangeable past and experience little or no freedom. The pastoral caregiver can start like this: “How do you want your life to be different one month (three, six, or nine months) from now? Be realistic – take into account your family, your finances, etc. Be very concrete and specific.” There is good reason for encouraging the cared-for to choose a specific objective and to work solely on that one task. Change, as Richard Wells noted, “is most likely to ensue from a concentrated focus on a single but significant problem in living and, conversely, the belief that much natural problem solving is weakened by attempting to deal with too many difficulties simultaneously.”[35] Narrowing the focus to one small objective increases the likelihood of positive change.
Setting goals and achieving them will provide an agenda for the terminally ill to be actively engaged in life. Completion of unfinished business while still alive is an important goal. The caregiver can creatively help to make this possible. While travel may be out of the question, other strategies can bring the destination to the dying. Perhaps, the book they always thought they would write is no longer possible, but the making of a video or audio tape to record their thoughts, experiences, and knowledge might serve as a substitute. These may be small goals perhaps, and short term goals, but they can build hope and engage the terminally ill in the normal daily tasks of living. Furthermore, an important legacy can be left behind for their loved ones, who may also be searching for meaning themselves after their loved ones die.
Cultural Considerations
How should a caregiver proceed to foster hope and set the stage for a “good life” in the Chinese cultural context? The beliefs and values held by the cared-for should be honored if the cared-for are to find contentment within them. The caring-one can model a healthy respect for life, death, and nature, recognizing that life and death are both part of nature, and helping the cared-for to discover their own meaning of life and death in conjunction with their heritage and their particular historical situation or socio-cultural context.
In China, the family comes first. Many terminally ill patients have found meaning for their pain and suffering in the mutually loving and supportive relationships in the family. They are often concerned about the heavy financial burden their medical treatments have imposed on their loved ones. It is not uncommon to observe that much of their unfinished business centers on the needs of their families. The caregiver is well advised to include the family in whatever health care decision that has to be made. The first documented case of physician-assisted suicide in China speaks for itself in this regard. On June 23, 1986, Xia Su-wen, a 59-year-old female, was taken to Han Zhong 陝西省漢中市hospital (Shaanxi province) for treatment of an infection while suffering from cirrhosis of the liver. Even though her condition improved after several days of treatment, her condition worsened on June 27 and she kept crying out, “It’s so painful. I don’t want to live.” After Wang Ming-cheng 王明成, one of her sons, learned that his mother’s condition was “hopeless” on June 28, he asked Dr. Lian-sheng Pu 蒲連升, the attending physician, to give his mother an injection so that she could die without pain. Dr. Pu refused at first. After Wang implored Dr. Pu several times, Dr. Pu was persuaded to let nurse trainee inject 100 ml. of a compound at 9 a.m. on June 28, before which time Wang had signed a formal letter stating that “Family member requests euthanasia. Signed: Wang Ming-cheng (son).” Before Dr. Pu went off duty, he gave order for the night-shift doctor to give a further injection if Xia didn’t die. At 3 am. Xia was further injected with a 75 ml. of wintermin compound, and she died at 5 am. on June 29, 1986. Other children of Xia Su-wen 夏素文, who were not consulted before, sued Dr. Pu for killing their mother. Both defendants were eventually found “not guilty.” The story did not end there. In February 2003, Wang Meng-cheng, terminally ill with stomach cancer himself, had his own request for physician-assisted suicide turned down. The disease eventually killed him in August of the same year.[36]
We have also seen how the caring granddaughter can inspire and nurture hope in her grandfather by modeling a spirit of hopefulness.[37] It is through her filial piety, unwavering commitment with faithfulness and love, conscientiousness, diligence and undivided responsibility that hopefulness is conveyed to the cared-for, helping her grandpa to transcend his suffering and feel blissful and content. In such a caring environment, the “seed-like presence of that which is hoped for” was sown. [38] When souls touch, hope can be inspired or transplanted from the one-caring to the cared-for. Another way may be more indirect – possibly through an “osmosis-like” process. Nevertheless, the caring-one would be well advised to take the cue from the cared-for in finding out what are the goals that they would like to realize.
In China, dialogues about death and dying can be perceived as interfering with inner harmony, even though there is no well-documented “fear of death” arising from these dialogues. There is also no evidence that breaking the bad news to terminally ill patients does any harm.[39] Nonetheless, it is still a common practice among Chinese to avoid telling the painful truths to their loved ones afflicted with advanced disease with limited life expectancy. There is still a lingering fear that the truth would deprive the patient of hope. Thus, until the family members are prepared to embrace the stark reality, it will not be wise for the caregiver to provide any unsought information. The caregiver, however, needs to be alert to any manifestation of despair or apathy in the cared-for, which may be an indication that the truth has already been recognized. Despair and apathy have been described as enemies of hopefulness.[40]
It is not uncommon to see the hope of reconciliation, the last unfinished business of the dying, dashed by one party’s attempt to “save face” even at the patient’s deathbed. The caregiver is well advised to keep this in mind while caring for the terminally ill and family. “Saving face” is said to be of great importance to Chinese, Japanese and other Asian collectivist cultures, but it is valued in most other parts of the world. The phrase appeared in Chambers’s Journal in 1917: “The civilian native staff had bolted at the first sign of trouble, ‘going to report to the authorities’ being their ‘save face’ for it.” [41] Saving face means doing something to avoid shame or embarrassment, or making a move that preserves one’s reputation from harm. “Face” in this context refers to dignity, prestige, or standing in the eyes of others, and “face” is very important to the Chinese.
The majority of Chinese people this author has come across in the interviews were peasants and “urban poor” who were not well-educated or fully-employed. They were generally raised in an environment of ancestor and idol worship. Because of their close ties to family, they generally believe that their ancestors would protect them and bless them bountifully if only they would reciprocate by burning paper money and offering food to their ancestors in the nether world. Some of these believers viewed the Christian deity as “foreign devil,” and attributed any misfortune to this “evil spirit.” While it is all too easy to call them superstitious, one cannot help asking: “Who am I to pass judgment on them? What makes my religion ‘truer’ than theirs?” They too were desperately grasping for a straw of hope in coping with the vicissitudes of life. The caregiver needs to be sensitive to such diverse cultural complexities, and provide care with compassion, empathy, and open-mindedness.
Role of Physicians
Beside the family caregivers, physicians can also provide many opportunities for fostering hope in the terminally ill. Deborah Mitchell [42] suggests that physicians make three promises to dying patients and families. First is the promise thatpatients do not have to die alone, assuring them that they will not be abandoned. This assurance gives those around the patient meaning for their participation in the drama and also gives the patient meaning in continuing relationships with others. The second promise physicians can give is that no extraordinary means will be used to prolong life. This acknowledges the importance of human interactions and touch in place of machines and life-saving technology. Meaning shifts from one based on quantity to one based on quality. The third promise that physicians can make to patients is that they will be remembered. This provides meaning for the life they have lived and allows them to continue to have purpose by shaping those memories in the time that lies ahead.
It is true that any member of the care-giving team can make these promises. Deborah Mitchell merely suggests that the gift comes from a physician, because it may “carry additional credibility, legitimacy, and validation.”[43] Believing that one’s sense of self is not “gone,” but is still under construction, allows patients a chance to reflect on who they are and how they will be remembered. These three promises begin the process of helping dying people find new meaning and new hope to carry on.
Role of Hospice Programs
Even though mainland China does not have any organized hospice program that I know of, a word should be said here about the important role played by the hospice program. Where hospice is available, physicians can refer some of the terminally ill patients to this program. This move of patients from a “sick role” to a “dying role” is an important transition, beginning with the labeling of such individuals as “hospice patients” and with the program’s subsequent management of the drama of dying.[44] Hospice achieves a role transition through the use of props, management of the setting, and the creation of a new reference group. This drama does not infer that hope can only be redefined for those labeled “hospice patient.” However, “acceptance of the identity brings new expectations and creates a reference group to assist in the reformulation of meanings.” Hospice surrounds the patient with people who acknowledge and value the new identity, often protecting the dying person from those that see the situation as meaningless and hopeless. Hospice plays an important role by creating opportunities for the family to participate in the drama, thus giving them new hope. [45] The challenge for other palliative care practitioners is to create a similar role and to provide a reference group to support the drama and its resulting meanings. Re-definition of hope begins with those surrounding the patient.
This hospice approach is important not only for patients, but for the health care providers and family as well. One of the successes of hospice is that, from the initial entrance into the program, dying stands in direct contrast to previous experiences, and thus new meanings and expectations are established. While sympathetic to the needs of the patients, hospices do not present this situation as sad, but rather as an opportunity, one with promise. Old meanings attached to images of technologies, physician office visits, and curative attempts to restore health are replaced with images of comfort, family, choices, and decision-making. This honest, open discussion is most often met with relief by patients and families as they realize they no longer must participate in a drama where they are not fulfilling their role; the patients are not “getting well.” It is important that caregivers recognize, as the focus of hope shifts, wishes for cure need not be eliminated. Wishing and praying for a miracle cure need not be lost when hope is directed toward comfort and dying well. Miracles can happen and there is nothing wrong with wishing and praying for them. However, people’s lives must be helped to move on with new meanings that are not dependent on miracle cures.
Role of the Pastoral Caregivers
Saved for the last, but not least, is the important role of the pastoral caregiver. Donald Capps gives an excellent description of this in his book Agents of Hope: A Pastoral Psychology.[46] First he quotes a short narrative from John Bunyan’s classic work The Pilgrim’s Progress:
“The name of the friend who accompanied the hero Christian throughout most of his journey was Hopeful. As Christian entered the River Jordan to the Promised Land, the last stage of the journey, he felt himself sinking and cried out to Hopeful, “I sink in deep waters, the billows go over my head, and the waves go over me.” Hopeful responded, “Be of good cheer, my brother, I feel the bottom, and it is good.” But Christian continued to cry out to Hopeful, convinced that he would die in the river and never gain entrance to the gate of the city. As he sank deeper and deeper, it was all that Hopeful could do to keep his friend’s head above water. When Hopeful comforted him, saying, “Brother, I see the gate, and men standing by to receive us.” Christian replied that it was not himself but Hopeful for whom they were waiting. But Hopeful persisted, telling Christian that his troubles and distress were not signs that God had forsaken him. He encouraged Christian to be of good cheer, for Jesus Christ is even now making him whole. With this, Christian broke out in a loud voice, exclaiming that he could see his Lord again and could hear Him telling him, “When you pass through the waters, I will be with you; and through the rivers, they shall not overflow you.” At that very moment, Christian found that the ground underneath him was solid, and as the river at this point was shallow, the crisis was over. Both men reached the other shore and were met by two Shining Ones who had been sent to minister to those who were soon to be welcomed into the house of salvation.” [47]
Then Donald Capps continues:
“Without Hopeful, Christian would surely have drowned. Without Hopeful’s encouraging presence, he would have succumbed to despair. Hopeful then is a powerful image of the pastor, as the one who gives assurance that all will be well; that when others sink, they will feel the solid ground beneath them; and that when their lives have fallen apart, Christ is even then at work to make them whole. Hopeful is not the one who makes Christian whole – only Christ is able to do this – but is the one who holds his friend’s head above water so that he can see his Christ and hear His promises. To be an agent of hope is what pastoral care is inherently and ultimately about.” [48]
I agree with Donald Capps that we, as pastoral caregivers, are agents of hope: not because we should be, but because we want to be; not because of our needs, but because of others’ needs; not because of our own agenda, but because of what the others desire. If hope is the perception of a realizable good in a promising future,[49] hope can be inspired and nurtured in the terminally ill within a caring atmosphere. When souls touch, hope can be transplanted from one hopeful person to another. Just as hope develops in the child and in the mothering person, mutual trust and love between the cared-for and the pastoral caregiver will also foster mutual hope. Everyone benefits.
As pastoral caregivers, we represent the God who is both with us and out in front of us calling, inviting, even challenging us to move into this future. As Jürgen Moltmann puts it, “God is the one who accompanies us and beckons us to set out. And it is God who, so to speak, waits for us around the next corner…Even on the false paths we take in life God continually opens up surprisingly new possibilities to us.”[50] “The living God does not beckon from behind, trapping us in history, but pulls us toward the horizons of promise and fulfillment,” says Andrew Lester.[51] We, in our frailty, must look beyond our immediate necessities or past liabilities, and anticipate the future with the awareness that we have freedom – however limited – to actualize who we ought to become. We bear the responsibility for shaping that future. As pastoral caregivers, we have the opportunity of pointing our terminally ill to this deeper level of hope. Perhaps there is no better way to convey this than to let them see it in the way we interact with them. The hope we share with them is likely to bring forth hopes of their own. Let them see the hope in our eyes.
Where There is Hope, There is Life [52]
The story of Mr. Li at the beginning of Chapter Two underscores the dilemma terminally ill patients with pain and suffering are facing in China: to live or to die. Their stories were heart-rending. I doubt if I have the answers to many of their questions and their problems. I believe that the answers lie within themselves, to be discovered or created when conditions are ripe. I believe that each person may find a different meaning in life at different times, different places, and different circumstances.
In my literature review, I have been impressed by what Viktor Frankl proposes – the will to meaning – that helps to sustain the lives of those who feel powerless to change their circumstances. Even though he was writing about the inmates of the Nazi concentration camps, his proposal also makes a lot of sense in the terminally ill. Building on his notion, I submit that hope may provide the terminally ill with a positive attitude to remain engaged in life even in the darkest of times. Hope allows one to project into the future for positive meaning in the present. I submit that, when the terminally ill seriously consider suicide, hope may deter them from such an act.
My review of current literature has revealed that not only can hope rest in meaning, it can also rest in love and support, in faith and trust, and in goal-setting and goal-attainment. The four dimensions of hope – experiential, relational, spiritual and rational – appear to be uniquely suited to deal with the existential concerns that are commonly found in the terminally ill: meaninglessness, isolation, groundlessness, and death. Hope has also been described as the first virtue (or human strength) that develops in the human life cycle. To the extent that strengths build upon prior strengths, this means that hope is the basis for all other human strengths.
Hope, as vision, also takes on different colored lenses according to varying cultural and communal contexts. The Chinese and Western perspectives on meaning and hope bring to light some of our hidden agenda, assumptions and presuppositions in our own tradition, while enriching each other’s tradition. This exchange of ideas and access to more options in fostering hope may prove beneficial to the terminally ill in coping with their suffering.
When I say “where there is hope, there is life,” I am referring to life in its totality: the life of the embodied soul and the relational self. There are some evidences to suggest that hope would provide the terminally ill a positive attitude to remain engaged in life, a better quality of life, relief of psychological distress, and more effective coping in their suffering. Further contribution from the new field of “biology of hope” indicates that certain immunological measures can be improved and life expectancy can be even lengthened in cases where hopefulness is cherished. It should be pointed out with caution that this thesis proposed here remains an untested hypothesis, and more research work will need to be done to establish its validity.
Thesis aside, it is the human story that will stay in our hearts. The story of hope is the story of perils and promises, of tragedy and beauty, of torment and goodness. Let us consider the case of the dying grandfather.[53] He had accepted the fact that his life would soon come to an end. The world seemed so grim and the future so bleak. The pain was getting unbearable. Money was running out. He had concluded that nobody else in the family but his granddaughter cared about him. He wondered: “What’s the point? What’s the use of fighting a losing battle? What’s the meaning and purpose of my life?”
Yet, while hitting rock bottom and in the throes of struggling, his eyes were opened to new possibilities. Yes, there was goodness in his life: the love and loyalty of his granddaughter, who had committed unwaveringly to his care. There was even meaning in his suffering. Through this ordeal, grandfather and granddaughter were closer to each other than ever before, and each was hopeful that her/his need could be satisfied by the other. The grandfather needed to be loved and cared for, and the granddaughter needed to be accepted without gender bias.
When the grandfather contemplated suicide, he reminded himself that he was not to abandon his family and blemish the family name. His belief in an afterlife in which he expected to give accountability for his life dissuaded him from committing suicide. Instead, he chose a positive stance: he looked to the future and acted accordingly. He looked for his long lost brother, not so much for reconciliation, but to satisfy his curiosity to see if the family name could be passed on. He hanged on to life, hoping to see a grandson conceived and born. Blood lineage and family legacy were matters of prime concern to him, and had given him reason for living.
It is a beautiful story, with a good ending. Grandfather finally discarded his prejudice against girls, and thanked his granddaughter heartily for her filial piety and loyalty. They had found each other. There was healing. Their hope of reconciliation had been realized. She got her acceptance and he had his contentment. He died peacefully.
The story did not end there either. Three years later, she turned blind with a congenital retinal condition. She wanted to kill herself. “No,” she told herself, “Killing oneself would only bring shame to the whole family.” Those were the words of her grandfather before he died. Even when everything appeared dark as night, she saw a glimmer of hope and a chance for thanksgiving. She found her peace in Jesus Christ. “Despite my blindness, I am thankful that I can still make a decent living and earn respect as an acupressure practitioner…I no longer envy those who have good health. A healthy person may not have a healthy heart.” Obviously, matters of the heart were more important to her than afflictions of the body.
In this story, the granddaughter was an
agent of hope too. She helped
her grandfather construct new meanings and redefine hope when the hope of cure
was beyond reach. She assisted him to appreciate life and allay fears about
death. She worked with physicians to establish promises of comfort, surrounded
him with love and support, helped him take an inventory of relationships,
shared with him her own faith, and created for him a safe environment to nourish
his hope. As a family caregiver, she nurtured her grandfather in body, mind and
spirit: through labors of love; support and caring; modeling hopefulness with
her unwavering commitment, conscientiousness, diligence and responsibility; as
well as encouragements, reconciliation, and healing. Because of her
hopefulness, and the hope that she inspired and nurtured in her grandfather,
her grandfather did not give up on living. He continued to engage in life. No
one knew for sure if this hope had lengthened his life, but one thing was for
sure, he had found meaning and purpose in his life, his reasons for living. The
words of Victor Richards ring true here: “The quantity and quality of care that
a dying patient receives are powerful adjuvants to the growth of hope, of
openness to whatever future may be his.”[54]
In return, the granddaughter’s hope also materialized. They both gave up the
idea of committing suicide. It is hope that displaces despair and apathy, and
fills the heart with faith and love. Indeed where there is hope, there is life.
When people have learned how to live with hope in the face of pain and
suffering, then physician-assisted suicide is less of an issue.
[1] Walter R. Fisher, “Narration as Human Communication Paradigm: The Case of Public Moral Argument,” Communication Monographs 51 (1984): 1-22.
[2] Friedrich Nietzsche, The Gay Science, trans. Walter Kaufmann (New York: Vintage Books, 1974), 4-5.
[3] This quote comes from Andrew D. Lester, Hope in Pastoral Care and Counseling (Louisville: Westminster John Knox Press, 1995), 27. Publication information for Jean-Paul Sartre not provided.
[4] Andrew D. Lester, Hope in Pastoral Care and Counseling (Louisville: Westminster John Knox Press, 1995), 30.
[5] Theodore R. Sarbin, “The Narrative as a Root Metaphor for Psychology,” in Narrative Psychology: The Storied Nature of Human Conduct, ed. Theodore R. Sarbin (New York: Praeger, 1986), 8.
[6] Stephen D. Crites, “Narrative Quality of Experience,” Journal of the American Academy of Religion 39 (Sept. 1971): 291.
[7] Stephen D. Crites, “Narrative Quality of Experience,” Journal of the American Academy of Religion 39 (Sept. 1971): 291.
[8] Hannah Arendt, The Human Condition (Garden City, NY: Doubleday & Co., 1958), 181.
[9] Dorothy Wholihan, “The Value of Reminiscence in Hospice Care,” American Journal of Hospice and Palliative Care 9 (1992): 33.
[10] Erik H. Erikson, Identity and the Life Cycle (New York: International Universities Press, 1959), 98.
[11] E. Mansell Pattison, “The Experience of Dying,” American Journal of Psychotherapy 21 (1967): 32-43.
[12] Arthur W. McMahon and Paul J. Hudick, “Reminiscing: Adaptational Significance in the Aged,” Archives of General Psychiatry 10 (1964): 292-98.
[13] Dorothy Wholihan, “The Value of Reminiscence in Hospice Care,” American Journal of Hospice amd Palliative Care 9 (1992): 33-35.
[14] Robert N. Butler, “The Life Review: An Interpretation of Reminiscence in the Aged,” Psychiatry 26 (1963): 65-76.
[15] P.G. Coleman, “Measuring Reminiscence Characteristics from Conversation as Adaptive Features of Old Age,” Int. J. Aging and Human Development 5 (1974): 281-294.
[16] Ibid., 283.
[17] Richard Bandler, John Grinder,Steve Andreas and Connirae Andreas, ed. Reframing: Neuro-Linguistic Programming and the Transformation of Meaning (Moab, Utah: Real People Press, 1982), 5-8.
[18] For a summary, see Donald Capps, Reframing: A New Method in Pastoral Care (Minneapolis: Fortress Press, 1990), 11.
[19] Andrew Lester, “Helping Parishioners Envision the Future,” Strategies for Brief Pastoral Counseling, ed.Howard W. Stone (Minneapolis, MN: Fortress Press, 2001), 50-52.
[20] Story of Mr. Li from Interview #6, Appendix.
[21] Andrew D. Lester, “Helping Parishioners Envision the Future,” in Strategies for Brief Pastoral Counseling, ed.Howard W. Stone (Minneapolis: Fortress Press, 2001), 52.
[22] Andrew D. Lester, Hope in Pastoral Care and Counseling (Louisville: Westminster John Knox Press, 1995), 29.
[23] Andrew D. Lester, “Helping Parishioners Envision the Future,” 52.
[24] Richard A. Gardner, Psychotherapy with Children of Divorce (New York: Jason Aronson, 1976), 58-59.
[25] Joseph E. Shorr, Gail E. Sobel et al., eds. Imagery: Its Many Dimensions and Applications (New York: Plenum, 1980), 253-66.
[26] The cared-for are invited to record whatever imagery experiences come to them, whether fleeting images or extended dramatic scenarios, whether seeming foolishness or with obvious associations, whether sleep dreams or waking imagery. Have these recorded in their journals without judgment and without censorship. This is one example taken from Ira Progoff’s book The Dynamics of Hope: Perspectives of Process in Anxiety and Creativity, Imagery and Dreams (New York: Dialogue House Library, 1985), 230.
[27] John Keats, “Sonnet.” In The Poetical Works of John Keats, ed. H. Buxton Forman (London: Oxford University Press, 1931), 486.
[28] Deborah Parker-Oliver, “The Social Construction of a Dying Role: The Hospice Drama,” Omega – Journal of Death and Dying 40, no. 4 (2000): 19-38.
[29] Ira Byock, “Steve’s Story,” in On Our Own Terms: Moyers on Dying Discussion Guide (New York: Thirteen/WNET, 2000), 8.
[30] Henri J. M. Nouwen, Out of Solitude: Three Meditations on the Christian Life (Notre Dame, IN: Ave Maria Press, 1974), 34.
[31] Dona J. Reese and Dean R. Brown, “Psychosocial and Spiritual Care in Hospice: Differences between Nursing, Social Work, and Clergy,” Hospice Journal 12, no. 1 (1997): 29-41.
[32] Steve de Shazer, Putting Differences to Work (New York: W. W. Norton, 1991), 113.
[33] Ben Furman and Tapani Ahola, Solution Talk: Hosting Therapeutic Conversations (New York: W. W. Norton, 1992), 91-106.
[34] Ben Furman and Tapani Ahola, Solution Talk: Hosting Therapeutic Conversations (New York: W. W. Norton, 1992), 102-103.
[35] Richard Wells, Planned Short-Term Treatment (New York: Free Press, 1982), 10.
[36] Yan Qin, “Schiavo’s Fate Fires Debate on Euthanasia,” China Daily (Mar.23, 2005), http://www. chinadaily.com.cn/english/doc/2005-03/23/content_427546.htm (accessible May 14, 2008).
[37] Interview #7, Appendix.
[38] Paul Tillich, “The Right to Hope: A Sermon,” Christian Century 107, no 33 (Nov. 14, 1990): 1064-67.
[39] Tse, Chun-yan, Alice Chong, and Janet Sui-yee Fok, “Breaking Bad News: A Chinese Perspective,” Palliative Medicine 17 (2003): 339-43.
[40] Donald Capps, Agents of Hope: A Pastoral Psychology (Minneapolis, MN: Fortress Press, 1995), 99. Shame is described as the third enemy of hopefulness.
[41] James Rogers, The Dictionary of Cliches (New York: Ballantine Books, 1985).
[42] Deborah R. Mitchell, “The “Good” Death: Three Promises to Make at the Bedside,” Geriatrics 2, no. 8 (1997): 591-92.
[43] Deborah R. Mitchell, “The “Good” Death: Three Promises to Make at the Bedside,” Geriatrics 2, no. 8 (1997): 592.
[44] Deborah Parker-Oliver, “The Social Construction of a Dying Role: The Hospice Drama,” Omega – Journal of Death and Dying 40, no. 4 (2000): 19-38.
[45] Deborah Parker-Oliver, “The Social Construction of a Dying Role: The Hospice Drama,” Omega – Journal of Death and Dying 40, no. 4 (2000): 19-38.
[46] Donald Capps, Agents of Hope: A Pastoral Psychology (Minneapolis: Fortress Press, 1995), 3-4.
[47] John Bunyan, The Pilgrim’s Progress (New York: Washington Square Press, 1957), 151-52.
[48] Donald Capps, Agents of Hope: A Pastoral Psychology (Minneapolis: Fortress Press, 1995), 3-4.
[49] Ibid.,4.
[50] Jürgen Moltmann, Foreword to The Origins of the Theology of Hope by M. Douglas Meeks (Philadelphia: Fortress Press, 1974), x.
[51] Andrew D. Lester, “Helping Parishioners Envision the Future,” in Strategies for Brief Pastoral Counseling, ed.Howard W. Stone (Minneapolis: Fortress Press, 2001), 58.
[52] This phrase is, to my knowledge, first used by Robert L. Richardson, “Where There is Hope, There is Life: Toward a Biology of Hope,” Journal of Pastoral Care 54, no. 1 (Spring 2000): 75-83.
[53] Interview #7, Appendix.
[54] Victor Richards, “Death and Cancer,” Death: Current Perspectives, ed. Edwin S. Shneidman (Palo Alto, CA: Mayfield Publishing, 1980), 479.
Appendix: Interview Data
APPENDIX: Interview Data
| Number | Age | Gender | Terminally ill patient | Family Member | Spiritual Counselor | Faith |
| 1 | 50+ | Male | No | Husband | None | |
| 2 | 50+ | Male | No | Son | Christian | |
| 3 | 30+ | Female | Yes | Christian | ||
| 4 | 60+ | Female | Yes | Christian | ||
| 5 | 30+ | Female | Yes | Christian | ||
| 6 | 40+ | Male | Yes | None | ||
| 7 | 30+ | Female | No | Daughter | Christian | |
| 8 | 70+ | Male | Yes | Christian | ||
| 9 | 50+ | Female | Yes | Christian | ||
| 10 | 60+ | Female | Yes | None | ||
| 11 | 70+ | Female | Yes | Christian | ||
| 12 | 30+ | Female | Yes | None | ||
| 13 | 90+ | Male | Yes | Christian | ||
| 14 | 18+ | Male | Yes | Christian | ||
| 15 | 70+ | Male | Yes | Christian | ||
| 16 | 40+ | Female | Yes | Christian | ||
| 17 | 30+ | Female | No | Daughter | Christian | |
| 18 | 40+ | Female | Yes | Christian | ||
| 19 | 40+ | Female | Yes | Christian | ||
| 20 | 20+ | Female | No | Daughter | Christian | |
| 21 | 40+ | Male | No | Yes | Taoist | |
| 22 | 40+ | Female | No | Yes | Buddhist | |
| 23 | 50+ | Male | No | Yes | Islamic |
In the following descriptions, all names used were fictitious to maintain confidentiality.
1. Mr. Zhou was interviewed in Sha-xi at 9 am. His wife with terminal colon cancer had just passed away at 5 am that same day, Dec.4, 2007. Duration of Visit: 60 min.
- Mrs. Zhou had suffered from nausea and vomiting, intractable pain and being bedridden, as well as anorexia and hematemesis (vomiting blood).
- 4-5 months of terminal suffering (uninformed of her prognosis before then)
- Husband (Age 50+) attempted suicide 4-5 months ago (he had past history of hallucinations more than 10 years ago) when he could not deal with it all
- Some of their neighbors and relatives were giving them unsolicited advice; he described them as “nuisances”
- His wife became more and more alienated from other people as she got sicker
- Meaning of life/death? Her three daughters were her whole reason for living
- Because of the illness, the family grew closer together
- Death was considered inevitable by her
- Before she received the bad news of her prognosis 4-5 months prior, she had already accepted Christ
- The church gave her much support, together with support from her family
- She had no more fear of death from then on (and same for her husband)
- She had accepted death, and was coping as best as she could until her granddaughter was born
- She died 17 hours later
Summary: A 50+ male was interviewed shortly after his bedridden wife had just died from colon cancer 6 hours ago on Dec. 4, 2007, following a protracted illness with intractable pain, poor appetite, nausea, and vomiting up blood. Husband attempted suicide 4-5 months ago when he was unable to deal with it all. Quotes from husband included the following:
“My wife was not told of the true nature of her illness until the very last few months of her life. Until then, the burden on the rest of us was suffocating us.”
“Many so-called friends gave us a lot of unsolicited advice that added to our burden. Why can’t they leave us alone?”
“With my wife’s illness, I have never felt so powerless before in my life, not knowing how long her suffering would last…For me, seeing her suffer had taken a toll on me. It was worse than my own pain.”
“My wife and I have embraced our daughters with love and joy, and we took pride in the harmony and security of our home.”
“The love of our three daughters have given us the reason for living. Their love for their mother gave her spirit a real boost.”
“The fact that our daughters would sorely miss their mother had given her the zeal to live. She missed them terribly. As long as she was alive, she wanted to spend as much time with them as possible.”
“I miss her. Who wants to lose someone you love?”
“I cared for her as best as I could.”
“Even when she was prepared to die, there was still much anguish and fear (of the pain). She yearned to be free from pain and suffering.”
“I stayed with her throughout this ordeal. I didn’t want her to feel alone.”
“Sometimes I sat with her in silence. She knew I was there with her.”
“We understand that suffering is inevitable. It can happen to anyone.”
“Her newly-found faith in Jesus Christ and the assurance of eternal life gave her hope to carry on.”
“The church provided us with a lot of support.”
“I don’t know if my optimism had done her any good, but the hope she hang onto had made her suffering in the last days more tolerable.”
“My wife’s desire of seeing the birth of our first granddaughter kept her going. This hope lifted her spirit, and alleviated her pain. It kept her actively engaged in whatever time that still remained.”
“My wife died peacefully seventeen hours after our granddaughter was born. It was a truly ‘good’ death” (I asked him what that meant. He replied, “She is resting in peace with the LORD now”).
“All my life, I have struggled simply to survive. May be my one purpose in life is to find a meaning for all this rat race, and all these obligations and duties!”
“I have done my best to provide for my family and sought betterment for their lives.”
“As I get older, I ask for nothing more but a lightened load to carry and an even lesser burden to others!”
2. Mr. Zheng was interviewed on Dec. 4, 2007 in Sha-xi in Guangdong. Duration of visit: 45 min.
- His Dad, Mr. Zheng, Sr., was suffering from lung cancer and could hardly see nor attend our interview.
- Dad was short-of-breath on exertion; had pain that needed narcotic injections every 2 days for its relief; and anorexic (without appetite)
- One daughter and one son (Yu-jia) was taking care of him
- One younger daughter who was living in Guangxi had planned on receiving Mom there when Dad eventually passed on.
- Emotionally, Dad was very aggravated; had a major row with the oldest son in Guangxi about how the children would be taking care of Mom at her old age; also worried about his son’s financial situation, especially when the family car recently had extensive fire damage.
- Dad was described as being very tough, having gone through many difficult times during the Chinese Cultural Revolution in the 60s and 70s.
- The doctor had given up on Dad’s chance for recovery, but Dad had not been informed as yet, although Mom knew.
- With money being tight, Mr. Zheng felt guilty for not taking his Dad to the hospital.
- Since accepting Christ, Dad felt a new birth. The church was very supportive.
- Since Dad almost died three years ago from his lung cancer, he was grateful for having been given a new lease in life.
Summary: A 50+ male was interviewed. His father, who was in constant pain from terminal lung cancer, was concerned about his son’s ability to pay for his medical care, and the discord among his children. Here are some quotes from the son Mr. Zheng:
“The doctor said that my Dad’s cancer is now terminal. My Mom and I decided not to tell him this, just to keep his hope alive. What’s the point of telling him? He is prepared for the worst anyway, and has taken care of all his unfinished business.”
“I feel guilty for not taking Dad to the hospital. The doctors told us that there was nothing they could do for him” (especially when the family financial resources were tight)
“Our relatives don’t understand. They chided me for not taking him to the hospital.”
“Dad understands. He is concerned about the expenses.”
“I let him talk. I just listened, trying to hold back my tears sometimes. I guess I can never really feel the way he feels, but at least he knows that I care.”
“He told me some of the things he was proud of, but also some of the things he regretted. I helped him to sort these out, and this had apparently given him some peace.”
“Whenever possible, I still maintain a daily routine for him. This has helped to distract him from his discomfort and pain.”
“I told him that it takes more courage to live than die. I encouraged him to finish the race with dignity, and he is doing that.”
“His courage has made us children real proud.”
“Dad was a new person after he almost died from his lung cancer three years ago. Life has a special meaning for him now.”
“He believes that God alone determines when he lives or dies. His faith seems to rekindle his will to live.”
“He is thankful for the gift of life from God. He realizes that life should be cherished.”
“Dad is also thankful for the support of the family and the church.”
“Dad and I both know that God will take good care of us no matter how tough our circumstances are. We believe that all things will work for the good of those who love the LORD.”
“Miracles can happen. They will never happen without faith.”
“Suffering can be a blessing in disguise. This ordeal has brought our family together. My sister in Guangxi is planning to have Mom stay with her when the time comes.”
“Dad now realizes that his life must have a purpose as long as he is still alive.”
3. Ms Du was interviewed in Sha-xi Dec. 4, 2007. Duration of visit: 40 min.
- Age 38, self-employed; divorced and living with her 10-year-old daughter and her very sick 68-year-old mother
- Ms. Du had throat cancer treated with surgery and post-operative radiotherapy, during which time she had to abort her pregnancy in order to facilitate the radiation treatment
- One uncle practiced feng shui風水; very superstitious; blamed her Christian faith (of a ‘foreign’ god) for causing the cancer
- She coped reasonably well with her own illness by a mix of optimism, strength of character, perseverance, forgiveness (forgiving the doctor who, she felt, was not competent in her care) and the belief that God walked wit her during her times of need
- Despite her own poor health, she tried her best to care for her mother, who was also very sick
- She had felt guilty for not looking after her father when he was dying from liver cancer. This made her decide to look after her sick mother as best as she could.
- She was thankful for having been provided with adequate health insurance
- Ling-zhu had accepted suffering as being inevitable and unavoidable.
- She believed that suffering can happen to Christians and non-Christians alike, and in her case, her faith was strengthened by all her sufferings
Summary: A 30+ female, mother of a 10-year-old girl, was recently treated for laryngo-pharyngeal cancer post-operatively with radiotherapy because of spread. She had been looking after her 60+ widowed mother (#4 interviewee) who was suffering from a chronic debilitating illness.
“With the radiotherapy, I had to pay the dear cost of losing my second pregnancy.”
“Even though my brother and my sister would have nothing to do with my Mom’s protracted care, I feel it’s my duty to look after her. My father died of liver failure at a time when I was powerless to help. Now I am in a position to help my Mom.”
“I feel that it is important for her to have the hope of eternal life. I have shared with her God’s promises to us as revealed in the Scripture. I have prayed that she can find faith, hope and love from knowing Christ. We have prayed together for healing, peace and comfort. We sang hymns together too. When all else fail, faith and hope sustain us.”
“Taking care of my mother has brought me closer to God.”
“I have learned perseverance, because I know God will look after all of us.”
“Now I have peace. My LORD and my God has strengthened me and walked with me.”
4. Mrs. Du, mother of Ms. Du, was interviewed in Sha-xi Dec. 4, 2007. Duration of visit: 40 min.
- Age 68; had a bladder fistula as a result of complications from gall bladder and bile duct surgery
- Looked tired
- Felt abandoned by both friends and family (by her son and her other daughter)
- Considered suicide once, but dissuaded by her daughter who offered a great deal of support and encouragement
- Family discord bothered her. The children were divided in their different levels of commitment to her care. Only Ms. Du, a devoted daughter, held on to look after her, while the other son and daughter did not care at all
- She appreciated her daughter Ms. Du a great deal
- In her opinion, Ms. Du had offered a great Christian testimony
Summary: A 60+ female widow, mother of #3 interviewee, suffered from inoperable post-operative complications that resulted in persistent urinary incontinence and recurrent life-threatening infections.
“I feel so embarrassed by the stench of my urine.”
“I don’t feel like having visitors anymore.”
“I wanted to die.”
“My family clan and fellow villagers cannot accept my daughter’s faith. They blame my illness on the fact that she is Christian.”
“My daughter tells me that if I give up now, others will surely say that my illness is the result of my wrong doings.”
“I am willing now to give life my best shot, while accepting suffering as being inevitable.”
“God has helped my daughter to live through her cancer. I am sure God will take care of me too.”
“I don’t feel abandoned anymore when I know that God walks with me.”
5. Ms. Liang was interviewed in Sha-xi on Dec. 4, 2007. Duration of visit: 40 min.
- Housewife in her 30s; 2 daughters – Ages 15 and 7
- Diagnosed to have throat cancer 6 months ago
- Spread had occurred; received 35 radiation treatments
- Waiting for chemotherapy
- Accepted Christ 3-4 years ago
- Embraced her suffering reasonably well
- Initially denied worrying, but then broke down when talking about her older daughter requiring surgery when they had no money to move ahead. This caused her a great deal of despair
- Her daughters’ future meant everything to her
- Husband came forward to help, including sewing and doing housework
- Her brother and her sister also helped with transportation
- Church family helped too
- She declined to say anything pertaining to meaning of life/death. Seemed to me that raising up her two daughters would mean a great deal to her in life.
- Hence, there was considerable apprehension in talking about death
Summary: A 30+ homemaker, mother of two girls, was overwhelmed by 6 months of radiotherapy for metastatic laryngo-pharyngeal cancer and the added burden of not being able to afford the cost of corrective surgery for her 15-year-old daughter’s “sunken chest” deformity. The mother had entertained the possibility of ending it all. She broke down with tears during the interview (I sat there with her, not knowing what to say. I handed her some tissue paper, and allowed her some space to recover before she continued):
“I’d rather die so that my daughter can live.”
“I feel so powerless whenever I think of my daughter’s future. There is so much uncertainty.”
“My husband has come to the fore to help me in my illness. He does the household chores including sewing!”
“My siblings also help with the transportation.”
“I may be hoping for too much, but I would like to see my two daughters grow up and become self-supportive.”
6. Mr. Li was interviewed in Wai-hai, Dec. 2007. Duration of visit: 30 min.
- Age: 40+
- Colon cancer dignosed in 2004; resected
- Cancer recurred in 2005; again resected
- Surgical complication in 2006: colostomy site prolapsed
- In Oct. 2007 (two months prior to this visit), his violent coughing led to severe low back pain that completely immobilized him
- Even needed help to roll over on his side
- Very distressed; no more financial resource to seek further chemotherapy or therapy for his back pain. He could not afford the bone scan that the doctor recommended
- Meaning of life? Stay alive for his daughter and his younger son, who was enrolled in technical education, about the equivalence of Grade 13, and very much determined to get further advanced training
- We (that is, including my contact who made the introduction) encouraged him to persevere (instead of giving up) and set a good example for his son
Summary: A 40+ male peasant, suffering from recurrent colon cancer the past 3-4 years, had been bedridden with severe low back pain. This pain first came on 8 weeks prior when he had a sudden coughing spell. He was taken to the hospital Emergency Room, where a bone scan was ordered. Since he could not afford the scan, he was told to leave the hospital (his voice broke down when talking about this, and he could not continue. I turned to the wife then, wondering what had happened):
“My husband was refused hospital admission, even though I knelt before his attending doctor, pleading him for compassion. You know what he said? ‘Sorry. No money, no compassion.’ What kind of doctor is that?” (At this point, the husband recovered and continued)
“I want to stay alive for the sake of my children. I don’t want them living in this cold and merciless society without a father.”
“If I simply stop fighting and kill myself, what kind of example am I setting for my children?”
As I said good-bye to this family, I had a very heavy heart. I contacted a friend of mine, a physiotherapist, to see if he could make a free house-call. Perhaps something could be done for this unfortunate family. My friend did come and offered this family his advice. When I returned in the Fall of 2008, I learned that Mr. Li had passed away)
7. Ms. Luo was interviewed in Jiangmen Dec. 2007. Duration of visit: 60 min.
- Age 30+ blind female from the farm in Northern Guangdong, brought up in a poor family of school teachers in two successive generations (her grandpa and her dad); worked in farm after Grade 7; poor health as a child with frequent colitis
- Her mother was the daughter of a landlord (an enemy of the Communist party); her father worked as a teacher in the city away from their home village
- Ms. Luo recalled her experience when she was 16, as the only caregiver for her 79-year-old grandpa in the last 6-7 months of his life, after his stroke that paralyzed him 18 months prior
- Both her parents were not available to share the work load. One uncle and one aunt stayed around to help some of the time.
- Grandpa was tough; tried to get up himself, but could not; incontinent most times
- He found it toughest to stand the indignity of being cleaned up by his granddaughter when he became incontinent
- He could be very irate, scolding her for little things like not getting him hot water on time
- One time he begged her to give him poison ‘cause he didn’t want to live any more. She didn’t comply with his wish. He eventually changed his attitude, believing instead that suicide would bring shame to the family. This helped Ms. Luo too when she once contemplated suicide herself
- She felt that Grandpa disliked her because she wasn’t the grandson he expected; she loved him nevertheless
- He thanked her at his deathbed; that made it all worthwhile for her
- Meaning of life for him? According to Ms. Luo, it would have been doing good and deceiving no one. Also it would be important to pass on the family name through blood line
- In his last days, he was hoping to find his long-lost brother to see if he had a son to pass on the family name
- For Ms. Luo, her vision started to deteriorate at Age 19, requiring her to stop work as a shopkeeper and instead do baby-sitting for her older sister
- Despite treatment, she became blind in her early 20s
- She became a Christian shortly after (in 2000). She read a Christian testimony that described God as a God of love and justice; she believed and got baptized in 2001.
- Once she almost died under the wheel; she believed that God must have saved her for a purpose
Summary: A 30+ blind female massage and acupressure practitioner recalled the time when she, as a sixteen-year-old, was the sole care-giver for her paternal grandfather in his late 70s who became paralyzed following a major stroke. Her own father had left the village to teach in the city, and her mother would have nothing to do with her father-in-law. Here are some of Ms. Luo’s statements:
“My grandpa was very irate and a most difficult person to care for. He was a good person though. He worked hard all his life for our family. He was just frustrated in not being able to look after himself.”
“I love grandpa dearly. I cared for him because he was my grandpa. I looked after him for 6 months when everyone else had given up on him.”
“In these months, I cleaned him up every time he lost control over his bladder and bowel. He found that very degrading.”
“In desperation, he once asked me to give him rat poison. While I could feel for him in his desperation, I just could not give him what he asked for.”
“He eventually changed his mind. He thought he would bring shame to his ancestors if he gave up on his family.”
“He realized that he would have to account for his earthly deeds even in his afterlife, which he believed.”
“It was so hard for me to please him. I wish he would treat me better.”
“He was hoping to have a grandson of his own to pass on the family name.”
“He was eager to make contact with his long-lost brother to find out if he had a son to continue the family name. If so, that would be a great relief on his guilt. Grandpa died without realizing his expectations.”
“Three years after my grandpa died, I was diagnosed as having a congenital eye condition that would make me blind. I had to give up a well-paid job and do baby- sitting for my older sister.”
“When I became completely blind, I felt like ending it all. It was at that time when my grandpa’s words came back to me. ‘Killing myself would only bring shame to the whole family.’ I followed that advice.”
“Despite my blindness, I am very thankful that I can still make a decent living an earn respect as a massage and acupressure practitioner to help people.”
“Now, I no longer envy those who have good health. A ‘healthy’ person does not necessarily have a healthy heart.”
8. Mr. Zhang was interviewed in Xin-hui City in Dec. 2007 with his wife Ai Yi in attendance. Duration of visit: 60 min.
- Mr. Zhang Age 72: divorced once, and now remarried
- 3 boys and 1 girl from previous marriage
- Ai Yi herself was a divorcee; quite a few years younger than Mr. Zhang; one son Age 22 from previous marriage, living with his father
- Mr. Zhang was getting short-of-breath and anorexic because of fluid in his lungs from heart failure; slept poorly with frequent wakefulness during the night
- Meaning of life? He believed that God is in control of his life. At a time when his own children from his first marriage turned him out of his house, it was his faith in God that prevented him from committing suicide, and it was God who blessed him with a wonderful mate like Ai Yi when he was in dire need of companionship
- He greatly treasured personal freedom and control in his life. Ai Yi once gave him a ride on her motorcycle when he felt really down. This made him feel good once again
- He confessed that he loved her more than his own family, including his children. They, just like his own brothers, rejected his plea for help when he needed that most, and they slapped on a lot of conditions before they would consider helping him
- Mr. Zhang had no grudge against God. Instead, he was thankful that God had provided enough money for him to pay for the medical treatment
- He had some regrets for being too kind-hearted, spoiling his two boys by doing everything for them
- He worried about how Ai Yi would survive financially when he was gone
Summary: A 70+ male suffered from terminal lung cancer with poor appetite, emaciation and severe shortness of breath. His four children and his ex-wife had evicted him from his own house, because he refused to “abide by their rules.” His long time friend in her 40s took him in and took care of him. He was appreciative of her compassion and caring.
“I felt really bad when my own family cast me out in my hour of need. She took me in. I would have killed myself if it wasn’t for her. She is my reason for living.”
“She used to drive her motorcycle and take me out for many outings in the country. I could feel free again.”
“I trust her. She is honest with me. She did not hide the truth from me about my illness.”
“Despite the pain, I hope to remain relatively alert and enjoy quality time with her as much as possible.”
“God always provides the best for me, and the best is yet to come – a heavenly place I can call home.”
9. Ms. Ou was interviewed in Xin-hui City in Dec. 2007. Duration of visit: 35 min.
- Age 50+: married
- One son who just graduated from Wu-yi University, and found a job close to home in Xin-hui City
- Ms. Ou was first diagnosed to have lymphoma 4-5 years prior, and had undergone both chemotherapy and radiotherapy
- Her disease had recurred, with more fluid accumulated in her abdomen (ascites) and legs; accompanied by frequent coughing but little pain
- The suffering from cancer had brought her closer to God
- While she was under chemotherapy 5 years ago, she came across a Christian chaplain who visited her frequently in the hospital. Despite the SARS (Severe Acute Respiratory Syndrome) at the time, this chaplain was not wearing a face mask. Such sacrificial love was an effective testimony in bringing her to the Christian faith
- Since then, her faith had given her much joy and thanksgiving despite tribulations
- The support from her husband, Mr. Huang, and her son was indispensable in her journey through her suffering
- She had accepted death and was fully prepared for that event
- She found contentment praying for others in need
Summary: A 50+ female was afflicted with advanced lymphoma spreading to the abdomen in the past year despite vigorous chemo- and radio-therapy. She suffered from a grossly distended abdomen and increasing difficulty in breathing. She had become a Christian since she witnessed the testimony from one of the chaplains in the hospital where she received treatment five years ago.
“My suffering had led me to Christ.”
“When the hospital chaplain came in to see me, it was during the time of SARS (Severe Acute Respiratory Syndrome) in Southern China. Everyone was wearing a face mask in the hospital, but she did not. Her selfless love for me made a big impact on me.”
“It’s my faith that has kept me going. No matter how rough the journey is, Christ is here with me.”
“My husband and my son were also very supportive.”
“I was hoping to see my son graduate. He did. Furthermore, I am thankful that he has found a job close to home. How wonderful!”
10. Ms. Zhou was interviewed in Jiangmen Dec. 2007. Duration of visit: 45 min.
- Age 61, husband Age 60; one son and two daughters, the older one being Ms. Yu, who was baptized over a year ago in Beijie Hospital where she was hospitalized. The daughter took us to see her mother
- Mother was noticeably short of breath and had been coughing for over a year. No significant physical pain
- Mother was not told that she had terminal lung cancer (metastatic, non-small cell)
- Daughter was concerned. She could not understand why her mother, who was not a smoker and did not have any family history of lung cancer, would have lung cancer. She was interested in knowing more about the effect of medication (Iressin) on her mother
- Mother was very troubled over her own health (she was teary-eyed) and concerned about the future
- Would like to see daughter getting married soon
- Husband was playing mahjong downstairs when we arrived at the house
- The whole family was very “caring” and “supportive”
- Meaning of life? Mother hoped to be able to return to the farm and work in the field, reaping the harvest
Summary: A 61-year-old female peasant, married with one son and three daughters, was afflicted with metastatic lung cancer, suffering from shortness of breath and coughing for over a year, but with no significant physical pain. Despite her initial attempt to avoid talking about her hurt, she became teary-eyed when she talked about her illness and her daughter’s future. She did not say a lot, but the little that she said touched me by its simplicity and authenticity.
“My one remaining desire is to see my eldest daughter getting married.”
“I love to return to the farm once more, to sow seeds and to rejoice in the harvest.”
11. Ms. Ye was interviewed in Xin-hui City Dec. 2007. Duration of visit: 30 min.
- Age 70+ female, a farmer all her life
- Suffering from diseases that had affected her spleen, bones and large bowels, giving her considerable pain in her splenic area
- She was hoping for a return to better health
- Family consideration was her priority
- She lived with her daughter, but she was constantly looking forward to her two sons visiting (the younger one being a Christian minister). They came to her house to have lunches with her
- Accepting life as it comes
- New found faith in Christianity
- Looking forward to seeing her grandchildren grow up (four in total)
Summary: A 70+ grandmother was thriving poorly with multiple medical problems (large spleen, chronic colitis, severe osteoporosis, etc.). When talking about her children and grandchildren, a sweet smile appeared on her face, replacing the agony she had been showing from her afflictions.
“I live here with my daughter, but I look forward to my sons coming here for lunch. I love to see their smiles.”
“Family is everything to me. My children have grown, and they have children themselves, but my children will always remain children in my eyes.”
“I just wish I can be healthy again to look after them.”
“I take each day as it comes.”
12. Ms. Zeng was interviewed in Xin-hui City Dec. 2007. Duration of visit: 60 min.
- Age 30+ female, self-employed, owner of hair salon; husband Mr. Ye also in his 30s; two daughters from husband’s previous marriage living with them, with mother-in-law helping out at home
- Second marriage for her too
- No religious commitment
- Ms. Zeng had a tumor removed from her right cheek a year ago, but this had recurred
- She was disappointed, but hoped that Chinese herbal medicine would help her
- Both husband and wife had found it important to have their say in health decisions
Summary: A 30+ female self-employed hair dresser was afflicted with recurrent lymphoma on her right cheek despite surgical resection. Her one daughter from previous marriage now lives with her ex-husband, and with her second marriage, she has two girls to look after in her household. Both husband and wife felt very much pressured by their respective families. The husband still felt guilty for succumbing to his siblings’ decision which ended in his father’s tragic death. No wonder, the wife felt strongly about making her own decision on her own health issue. I felt it was appropriate to let her vent out her feelings.
“This life is my life, wholly mine. I want to have the sole right to determine when and how I live or die.”
“I am still young. I am not supposed to have cancer. If there is a God who is love, why this torment? ”
“I want to live life to the fullest.”
“A high quality of life is very important to me.”
“I enjoy my life as a journey; never mind the destination.”
“I am disappointed that the lymphoma has come back. Now I am taking Chinese herbal medicines in the hope of fighting it off.”
13. Mr. Peng was interviewed in Xin-hui City Dec. 2007. Duration of visit: 45 min.
- Age 90; having a continuous cough that drained much of his energy as well as recurrent urinary tract infections
- Heavy smoker since his teenage years; likely to have lung cancer
- Lived alone; preferred control over his life
- Loved to see his grandchildren grow up
- Had been a long-time Christian
Summary: A 90-year-old male had a persistent cough, which was still undiagnosed. The cough had persisted despite antibiotic treatment, and this had given him many sleepless nights, draining much of his energy. He lived alone and had been independent all his life.
“I prefer living by myself. The children have their own lives to lead.”
“My children and grandchildren are supportive, but I don’t want to be a burden to them.”
“I have been a Christian all my life.”
“The way I understand suffering is that suffering can be redemptive, just as Christ has suffered for the forgiveness of our sins.”
“Through our suffering, we can empathize with those who suffer. Just as 2 Cor. 1:3-4 tell us, ‘we may be able to give comfort to others who are in trouble, through the comfort with which we ourselves are comforted by God.’”
“Thank God, there is hope in the midst of suffering. There will be light, and there is going to be a future when there is no more sorrow and suffering.”
“Christ’s values are my values. In Christ, I have found contentment in an abundant and eternal life. Heb.13:5 says it all, ‘Be content with such things as you have: for he (Christ) has said, I will never leave you, nor forsake you.’”
“I see my purpose in life as God’s purpose for me: to love – loving God, loving my own self, my family, my neighbors, my friends, my country, and my fellow men, even my enemies. I want to be more like Christ. I don’t want to be a hypocrite, saying one thing and doing another. I want to live out my faith – to be loving, humble, faithful, honest, and responsible.”
“As I experience God’s grace and God’s gifts in my life, I have grown spiritually. It has been my privilege to be both God’s servant and a witness to God’s glory.”
“I hope to be a good father and grandfather. I’d like to leave behind me an eternal legacy for my children and grandchildren. I keep praying for them to grow in Christ.”
“I am tired of living. I want to have a good death.”
“There is a time to be born, and a time to die. The seed must die before there is new life.”
“I believe that we are only sojourners on earth. Death is only a transition – like the caterpillar and chrysalis eventually giving way to a beautiful butterfly. Death is by no means the end – it is only a beginning. I believe in afterlife.”
“As the old saying goes, ‘Even a tiny ant yearns to live.’ How can I kill myself? God alone determines when and how I die.”
14. Mr. Xie was interviewed in Xin-hui City Dec. 2007. Duration of visit: 40 min.
- Age 18, male, the only son in his family
- Last year of high school; interested in computing science as career
- Afflicted with Congenital Bifurcate Aorta and Septal Heart Defect with absence of pulmonary artery to the left lung, resulting in small stature, cyanosis, and physical handicap (could not play basketball). Prognosis very poor
- Only chance for survival would have to be a heart-lung transplant, which would, however, carry a high operative mortality
- Emotionally, Mr. Xie appeared to be resigned to accepting the inevitable
- Willing to accept that God’s way might not be the way that one might wish for
- He was hopeful that future medical advances might turn things around for him
- He appeared to have strong faith in God, having been a Christian since Age 7 (when his grandma took him to church)
- Meaning of life? To him, life was very precious and a gift from God
- Life should be treasured, more so because of his poor health
- He was aware of his parents’ feelings of guilt for giving birth to a child with congenital heart disease
- His parents, uncle, and aunt all gave him good support
Summary: An 18-year-old male high-school student was afflicted with a congenital heart disease resulting in small stature and significant physical handicap. His only chance for survival was a heart-lung transplant, which, at the time, carried an extremely high mortality rate in China.
“I have peace in my heart. I have accepted the fact that my life expectancy would be inevitably short.”
“But, perhaps, future medical advances may improve my chance of survival.”
“My parents feel badly about giving me birth with this problem, but who can blame them?”
“I am grateful to my parents for raising me up.”
“They have given me much love and support, more than they realize. So have my uncle and my aunt.”
“My life comes from God. I treasure it dearly. For the past 11 years God had given me peace.”
“With God by my side, my burden is light.”
“Prayer gives me the power to live another day.”
“Where there is God, there is hope. My hope lies in eternity, knowing that God is with me, now and forever more. I am not afraid of death anymore.”
15. Mr. Liang, Sr. was interviewed in Wai-hai, Dec. 23, 2007. Duration of visit: 25 min.
- Age 70+, male; lived with his wife and his son
- His son recently underwent rehabilitation from drug addiction
- Mr. Liang, Sr. became bedridden because of severe pain since he fell on his low back two weeks ago.
- He could not afford the cost of pain relief
- He was hard-of-hearing, and was not talking much
- He said he was simply living from day to day for the moment
- He wished he could die, but what kept him going was the hope to see his son recover fully from the addiction and become once again a useful member of society
- He recently became a Christian, after his wife and his son made that commitment
- He received good support from his wife and from church members visiting him
- He claimed that he believed in life after death
Summary: A 70+ male fell on his low back a few weeks prior and remained bedridden, because he had no money to see the doctor for pain relief. His wife was looking after him. He had one son whose best friend saw me at church and invited me to visit this family, because the father was at the brink of committing suicide. There was a lot of despair as the father talked about his pain and suffering.
“I don’t want to live anymore with this pain. It is killing me.”
“I have thought of suicide, but I can’t do it, not while my son is still getting drug rehabilitation. I’d like to see him hold down a job and become once again a useful member of society.”
“For the moment, I just have to grit my teeth and simply live from day to day.”
“I have good support from my wife and from the church members ever since my son became a Christian during his drug rehabilitation.”
“Yesterday, he (pointing to his son’s best friend) shared the gospel with me. I find the concept of afterlife a very comforting thought.”
“I now believe.”
16. Ms. Sun was interviewed in Jiangmen Dec. 26, 2007. Duration of visit: 30 min.
- Age 40+ female; husband left her more than 10 years ago; one daughter (Age 23)
- She had lumpectomy for breast cancer; metastases were treated by chemotherapy
- Meaning of life? Nailing down a good job
- Grateful that daughter was so good to her; love from her daughter was very important to her
- She felt that her previous idol worship might have led to her breast cancer, and that this new found faith in Christianity would lead her to a cure
- She had not been baptized as yet
Summary: A 40+ female was recently treated for breast cancer with post- operative chemotherapy. She was a single parent, ever since her husband left her more than 10 years ago with a child to bring up all by herself. She felt strongly that her illness was somehow brought on by her idol worship. There was guilt that required resolution.
“Do you think that my idol worship had anything to do with my illness?”
“My friends told me that becoming a Christian would help me in my illness. Do you think that miracles can happen?” (At this point, I thought she needed some clarification, but I resisted the temptation to budge in and be her counselor. I encouraged her to continue praying to God for healing)
“I read about miracles in the Bible as a result of faith. I want to believe that. I pray daily. May be God will hear my cries for help and be merciful.”
“Thank you for helping me to understand that illness, like rain, falls on all people, good and bad.”
“As a matter of fact, because of my illness, my daughter and I have drawn closer to each other.”
“I try to lead a normal life as much as possible until the very end.”
“I am just thankful that I can still work part time.”
(When I left, I encouraged her to find a spiritual home where she would feel comfortable in, and continue to grow in her faith)
17. Ms. Hong was interviewed in Jiangmen Dec. 26, 2007. Duration of visit: 45 min.
- Age 30+ female; 3rd in sibling order among 4 girls
- She had one 9-year-old son, and a younger daughter
- The family came from Chao-zhou in Southern China, one of the first places heavily influenced by Christian missionaries from the West
- For that reason, she and her sisters were 3rd generation Christians
- Her father was severely injured in a motor vehicle accident in year 2000. Together with her mother and an older sister Yu, Ms. Hong worked hard to care for her father, who remained semi-comatose
- Their love and commitment had impressed the medical staff at the hospital
- What kept her father alive? I asked. Ms. Hong gave several reasons from her own perspective: (1) it could be his Christian faith; (2) it could be his love for his family, especially for his two-and-a-half year old grandson; and (3) it could even be personal dignity that he valued a great deal. This would explain why he wanted to die when this last straw was removed from him.
Summary: A 30+ female, mother of two (a 9-year-old son and a younger daughter), was the primary caregiver for her father, who remained semi-comatose following a motor vehicle accident. Her eldest sister was reluctant to offer a helping hand, and there were times when they had open arguments in front of their father. At that time, even though he could not respond in words, his tears were seen flowing down his cheeks. Afterwards, he tried to pull out his intravenous tubes. Another time when he indicated that he did not feel like living anymore was when he had to suffer the indignity of having his impacted stool evacuated digitally by his wife and his younger daughter.
“It was hard for him” (the daughter said). “For a long time afterwards, he refused to eat and would not respond to us at all.”
“I prayed many times to the LORD to take him home.”
“When my prayer was not answered, I started to give up on God.”
“It was then that I heard a small voice saying, ‘If you refuse to believe in me, would that help your problem?’”
“From that time on, whenever I strayed from God, this reminder would return again and again.”
“It was my father’s faith that gave him peace. I never once heard him complain.”
“Love kept him going. My father loved his grandson, who was just over 2 when my father died in 2000. Our family was his pride and joy.”
18. Ms. Huang was interviewed in Jiangmen Dec. 2007. Duration of visit: 30 min.
- 46-year-old single female afflicted by breast cancer in 2000
- Had surgical excision in 2001, followed by chemotherapy recently for recurrent disease
- Her mother passed away 9 years ago. She had been looking after her father.
- She had one younger sister who was very supportive
- At one time, she did not find any meaning to her life. Life was a constant battle, with emotional ups and downs
- She was afraid of death. Just thinking about her own death before her father’s made her very uncomfortable
- She had found solace in the chaplain’s counseling, as well as in nature and in prayers
Summary: A 40+ single female was afflicted with recurrent breast cancer for which she was receiving chemotherapy.
“I find solace in nature. I cherish my morning walks in the surrounding hills and woods.”
“When I am alone in the woods, I hear birds sing praises for each new dawn. I am blessed more than I ever know.”
“My close friends and my younger sister often cheered me up when I felt down. They are my best friends.”
“I still fear death. May be it is the way I have been raised.”
“I have been looking after my father ever since my mother died nine years ago. It disturbs me to think that I may die before my father does.”
”Prayers sustain me when I don’t feel like living anymore.”
19. Ms. Cao was interviewed in Jiangmen Dec. 2007. Duration of visit: 45 min.
- Age 40+ female with severe bronchiectasis (acquired from childhood) with recent 2-year history of hemoptysis that required frequent hospital admissions
- Past history of pulmonary tuberculosis over 10 years ago
- Her hypoxia had led to occasional lapses of memory
- She had two children, Age 12 and 13, both being excellent students in Grade 5 and 6 respectively
- Ms. Cao never married the father of her two children
- He was a married man, though he hid that fact from her at the time they lived together
- They were good financial partners, having once set up a company that eventually came under her name when he gambled away his share.
- He would come back now and then to see his two children
- He lived with Ms. Cao’s niece, with whom he had another child.
- Ms. Cao felt very ambivalent and powerless dealing with this relationship and with her own declining health
- She was brought to tears during the interview, fearing that she would die before her children would become independent
- This was particularly agonizing when she recalled that her own mother died while she was about 3- or 4-year-old
- Meaning of life? Bringing up her two children
- She found love and support from her children and from brothers and sisters in Christ
- She admitted that her faith was weak and that she tended to be impatient
- She said she didn’t know how to pray
- She expressed the hope that she could at least see her children grow to 18 or 19
Summary: A 40+ single mother of two children (age 12 and 13) whose father deserted them after his own wife found out about his extramarital affair, was suffering from chronic obstructive lung disease, coughing up blood in the past two years and suffering from memory lapses because of chronic anemia and hypoxia.
“There is not much I can do about my declining health.”
“I hope to see my children become independent, but I fear that I may not have long to live.”
“I was three years old when my own mother died, and it looks like…” (she could not continue, her eyes filled with tears)
“Both my children have given me a lot of loving support. This has kept me going.”
“My faith is still weak. I don’t know how to pray. Would you help me?”
(I taught her how to pray before I left)
20. Ms. Wu was interviewed in Wai-hai, Dec. 2007. Duration of visit: 45 min.
- Age 20+ single female from Western Guangdong Province
- Ms. Wu was involved in an accident a year ago in Guangzhou, sustaining extensive pelvic fractures
- Worse still, she recently lost her mother to renal failure
- Her mother was only 51, requiring multiple hemo-dialysis procedures to stay alive
- About five months ago, the doctors told Ms. Wu (through her older brother) that there was nothing they could do for her mother
- It was not a matter of money. It was because of her mother’s poor response to dialysis itself
- This medical opinion was kept from her mother who was discharged from the hospital, still hoping that dialysis would buy her more time. Ms. Wu knew that her mother was not going to make it
- On Dec. 19, Ms. Wu’s mother became very sick from the uremia, getting short of breath and having a lot of abdominal pain
- She asked Ms. Wu to take her to the hospital for more dialysis. Ms. Wu felt so powerless. It was a rough night with her mother and a heart-breaker for Ms. Wu
- Her mother finally passed away at home in the morning
- Ms. Wu felt a lot of guilt for “abandoning” her sick mother
- Other family members (uncle, etc) accused Ms. Wu of falling away from the traditional idol worship and they had attributed her family’s woes to her Christian faith in a “foreign” god
- According to Ms. Wu, it was renal dialysis that kept her mother’s hope high
- Another reason for living for her mother might be the unfinished business of seeing the youngest daughter come home before she died
- Ms. Wu admitted that her faith was still weak
- She could not understand why her mother had to suffer so much if God was compassionate
- Ms. Wu received little love and support from her own family
Summary: A 20+ single female was the primary caregiver for her 51-year-old mother until her mother’s demise from kidney failure.
“Most of our relatives in the clan were superstitious ancestor-worshippers. They could not accept my faith. They called my God ‘foreign devil.’ They believed that my faith had brought about this illness in mother.”
“My mother took this rejection by the relatives real hard. She became very isolated from them, even though she could not understand why she had to suffer.”
“She could not understand why I would not take her to the hospital. I still feel guilty about it.” (I did not understand that either, but I let her continue)
“The doctors at the hospital told me not to bring her back. They told me that nothing could be done for my mother.”
“We thought it best not to tell her what the doctors said, because that would devastate her. She would have committed suicide.”
“Her one desire was to see her runaway daughter come home. It was an issue that continued to bother her. She died before my sister came home.”
“When she was still alive, my mother used to enjoy gardening. The sight of new life springing up in the garden gave her spirit a real lift.”
21. A 40+ male Taoist priest was interviewed in Xin-hui, Dec. 2007. Duration of visit: 30 min. Questions pertaining to suffering, terminal illness, as well as choices of life versus death were posed to him. The following is a summary of some of his comments:
”Suffering is our human emotional response to frustrated desires. Natural disasters (such as tsunami, hurricane, earthquake, etc.) cause suffering because they destroy some of the values we treasure (life, property, security, etc.). When we become frustrated in our desires of a pain-free life, of love, of fame and fortune, etc., suffering ensues, including fear of a painful and early death, of rejection, of low self-esteem, of poverty, etc.”
“Our wise teacher Lao-zi once said, ‘We will not suffer if we can let go of our emotions and desires.’”
“Suffering can be a blessing in disguise, with crises turning into opportunities.”
“Faith, love, and hope can help.”
“We too often lack the audacity to go outside our box in dealing with our paradoxes. Hope will do just that, turning our eyes to future possibilities and expectations. The terminally ill should not be deprived of hope to survive the ravages of their illness and to have healing, if not cure.”
“The caregiver’s attitude should be no less hopeful. Hope is contagious. The caregiver’s love and unwavering commitment will inspire hope even in the terminally ill.”
“However, inspiring and fostering hope is unlikely to help if the patient doesn’t wish to live any more.”
“Instead of inspiring and fostering hope in the terminally ill, is it not better to nurture a healthy respect for natural death and for one’s responsibilities when alive?”
“Acceptance of impending death does not necessarily imply passiveness and despair. It can mean actively facing death with courage…” (he continued)
“…full of gratitude for a life well lived and worthy of celebration. This is the legacy we should leave behind.”
“The meaning of life varies with each individual, influenced by different cultures and backgrounds, and by different ways of life.”
“The purpose of my life is to be one with nature, and to continue the process of learning and growth in the way of the Tao. My goal is to learn how to be humble and to grow in self-restraint as I serve others in need.”
“Following the Tao will lead to a life full of joy, freedom and dignity – enjoying good health relating to one another, and in knowing ourselves.”
“I am against suicide, including physician-assisted suicide, but I do grant that it is a personal decision. Patients opt for this because they think they have no other choice, but there are in fact other choices.”
“It is very difficult for us as sons and daughters to consent to physician-assisted suicide involving our parents, even when requested by either parent. It implies that we have failed as children to provide for our parents. In China, filial piety comes first. Physician-assisted suicide in China involves not just the patient, but the whole family and community as well.”
“When I do counseling pertaining to the terminally ill, I try to help that person understand death. Death is natural. It’s part of life, and it is inevitable.”
“However, we should not take a fatalistic view of our suffering, and take it lying down. Each of us has the power to change our lives and grow out of our suffering.”
“I believe that natural death, rather than physician-assisted suicide, is a ‘good’ death. I prepare my counselee to face death with peace and dignity.”
22. A 40+ female physician of Buddhist faith was interviewed in Jiangmen Dec. 2007. Duration of visit: 30 min. Questions pertaining to suffering, terminal illness, as well as choices of life versus death were posed to her. In her professional capacity, she had provided medical care for many patients who suffered from terminal illnesses, but she had no personal experience of caring for any critically ill family member. The following is a summary of some of her comments:
“Suffering is a human perception, and its extent depends on one’s awareness and interpretation. Our fixation on bodily desires and our lack of wisdom result in suffering, according to the law of causality, karma.”
“Our follies will have to be paid for, either in this life or the next.”
“We suffer because we cannot free up our mind in our perception of pain. If we meditate on the Dhamma, truths taught by Buddha, we can tolerate pain a lot better and suffer less.”
“I help patients understand that suffering is a fact of life. Without tasting the bitterness, how can we appreciate the sweetness in life?”
“I tell my patients, ‘The world keeps changing, so will suffering. Suffering will come to pass, just as it arrives unexpectedly sometimes.’”
“Prayer helps in suffering. Prayer, for me, does not involve entreaties to Buddha. Instead, it helps me to cleanse my soul and open up my heart and mind to new possibilities and solutions.”
“Sometimes, I seek help from my priest.”
“The priest would suggest that my patient buy some captive fish or birds, and set them free so as to gain credit in the nether world.”
“It will be helpful to sort out some of the unfinished business in the terminally ill.”
“I would explore the patient’s own meaning of life, because it varies with individuals.”
“Hope may not relieve the pain, but it can relieve the suffering.” (“What do you mean by hope?” I asked) “Hope, in my books, is earnestly looking to the future with the anticipation of fulfilling one’s goals or desires. It is different from wishful thinking.”
“Life is nothing but part of an eternal cycle of birth and death. We Buddhists liken it to a spinning wheel, with transmigration of souls and incarnation. Life is like a flame burning bright. With death, the flame is snuffed out for the moment, only to be lighted elsewhere.”
“I hope that my life here on earth and hereafter can be cause for celebration.”
“I have been struggling for control of my own life and of others’. It’s about time that I should let that go. Buddha’s teaching has enlightened me and given me much peace.”
“I feel a strong responsibility toward my family and my country. A happy and harmonious family is very important to me.”
“My purpose in life is to realize my self, actualize my potentials, and use them to help others. One of my dreams is to learn as much as I can. Another one is to pursue all that is beautiful and good, including world peace, justice and goodwill.” (“What is good?” I asked)
“Ethics of good or bad, right or wrong, is entirely subjective, and varies with different cultures, religions, races, etc. It all depends on one’s sense of wisdom and self-realization, which will help one to find peace in the midst of suffering.”
“I believe compassion should come first. I am for physician-assisted suicide. If you put yourself in the shoes of those suffering from intractable pain in a terminal illness, and without the money to get pain relief, wouldn’t you want to end it all? Why prolong the misery?”
“Isn’t it enough burdens on the family already?”
“We have limited resources. The same resource in prolonging life for the terminally ill can be used for other causes, such as looking after orphans.”
“If I were in the same boat, I would forget about further medical treatment. I would spend my last days doing what I love to do. I would travel the world while I still can, and see more of this world before I die.”
“The key lies in the patient’s own attitude or perception toward this pain and suffering. When someone has lost the will to live, the battle is already lost. Though alive, this person is nothing but a walking corpse.”
23. A 50+ male of Islamic faith was interviewed in Guangzhou Dec. 2007. Duration of visit: 30 min. The life of his own mother was once sustained on long-term life-support systems. The following is a summary of some of his comments on questions posed to him regarding suffering, terminal illness, and choice of life versus death. Physician-assisted suicide came up in the discussion.
“It was tormenting me to see my mother deteriorate physically and mentally.”
“I did my best to provide comfort and support to my mother.”
“I gave thanks to Allah everyday, even when things looked bad, because they could be worse.”
“When my mother was alive, the sky was still blue; then it darkened when she died.”
“There is suffering in the world because the world deviates from Allah’s purpose and Allah’s ways.”
“Death itself should not be feared. It is merely a return to Allah.”
“I have learned from suffering. It draws me closer to Allah.”
“I knew I was hoping against hope, but I kept telling myself that nothing is absolute. Miracles can happen. They will not happen without faith and hope.”
“I continued to consult with the doctors. May be advances in medical sciences will catch up with my mother’s illness. Who knows?”
“I was not sure if I had done my mother much good, but at least my positive attitude made her suffering more tolerable and improved her quality of life in her remaining days.”
“There is always the hope of a better life after this one.”
“I believe that being alive already means a lot.”
“My purpose in life is to honor Allah and serve my fellow men.”
“Personally, I am against physician-assisted suicide, especially when it involves my mother. I want to honor her and pay her a debt of gratitude in return for her love. It will be hard for me to give up on her.”
Bibliography
Alsop, Stewart. Stay of Execution: A Sort of Memoir. New York: J. B. Lippincott, 1973.
Anderson,Ray S. Spiritual Caregiving as Secular Sacrament: A Practical Theology for Professional Caregivers. London: J. Kingsley Publishers, 2003.
Arendt, Hannah. The Human Condition. Garden City, NY: Doubleday & Co., 1958.
Bandler, Richard, John Grinder, Steve Andreas, and Connirae Andreas, eds. Reframing:
Neuro-Linguistic Programming and the Transformation of Meaning. Moab, UT: Real People Press, 1982.
Barer, Morris L., et al. “Aging and Health Care Utilization: New Evidence on Old Fallacies.” Social Science and Medicine 24, no. 10 (1987): 851-62.
Barth, Karl. Church Dogmatics. Vol. 2, pt. 1. Trans. G. T. Thompson. Edinburgh: T. & T. Clark, 1957.
Beavers, Robert, and Florence Kaslow. “Anatomy of Hope.” Journal of Marital and Family Therapy 7, no. 2 (April 1981): 119-26.
Bloom, Gerald, and Sheng-lan Tang, eds. Health Care Transition in Urban China. Aldershot, Hants, England; Burlington, VT: Ashgate, 2004.
Blumenthal, David, and William Hsiao. “Privatization and Its Discontents – Evolving Chinese Health Care System.” New England Journal of Medicine 353, no. 11 (2005): 1165-70.
Boisen, Anton T. The Exploration of the Inner World: A Study of Mental Disorder and Religious Experience. 2nd ed. New York: Harper & Brothers, 1952.
Bowman, Kerry W., and Peter A. Singer. “Chinese Seniors’ Perspectives on End-of-Life Decisions.” Social Science and Medicine 53, no. 4 (2001): 455-64.
Brueggemann, Walter. Hope within History. Atlanta: John Knox Press, 1987.
Buber, Martin. I and Thou. Trans. Walter Kaufman. New York: Scribner; Edinburgh: T. & T. Clark, I970-1.
Bunyan, John. The Pilgrim’s Progress. New York: Washington Square Press, 1957.
Butler, Robert N. “The Life Review: An Interpretation of Reminiscence in the Aged.” Psychiatry 26 (1963): 65-76.
Byock, Ira. “Steve’s Story.” In On Our Own Terms: Moyers on Dying Discussion Guide, ed. David Reisman. New York: Thirteen/WNET, 2000. http://www.pbs.org/wnet/onourownterms/community/pdf/discussionguide.pdf (accessed May 20, 2008).
Cameron, Miriam E. “Technical Problems Involving Death.” AIDS Patient Care: A Journal for Health Care Professionals 8 (Oct. 1994): 269-78.
Camus, Albert. The Myth of Sisyphus. Trans. Justin O’Brien. London: Penguin, 2000.
Capps, Donald. Agents of Hope: A Pastoral Psychology. Minneapolis: Fortress Press, 1995.
________. Biblical Approaches to Pastoral Counseling. Philadelphia: Westminster Press, 1981.
________. Reframing: A New Method in Pastoral Care. Minneapolis: Fortress Press, 1990.
Capps, Walter H. Time Invades the Cathedral: Tension in the School of Hope. Philadelphia: Fortress Press, 1972.
Carrigan, Robert L. “Where Has Hope Gone? Toward an Understanding of Hope in Pastoral Care.” Pastoral Psychology 25, no. 1 (Fall 1976): 39-53.
Charles, Robert H. A Critical History of the Doctrine of a Future Life in Israel, in Judaism, and in Christianity. London: A. & C. Black, 1899. Reprint, Whitefish, MT: Kessinger Publishing, 2007.
Chen, Jia-gui, and Yan-zhong Wang. “The Report on China’s Urban Health Care System.” In China Social Security System Development Report 1997-2001 [in Chinese]. Ed. Jia-gui Chen. Beijing: Shehui Kexue Wenxian Press, 2001.
Chen, Yu-hsi. “The Way of Nature as a Healing Power.” In Handbook of Multicultural Perspectives on Stress and Coping, ed. Paul T. P. Wong and Lilian C. J. Wong, 91-103. New York: Springer, 2006.
Cole, Thomas R. “Gaining and Losing a Friend I Never Knew: Reading Claire Philip’s Journal and Poetry.” Journal of Aging Studies 9, no. 4 (Winter 1995): 329-34.
Coleman, Peter G. “Measuring Reminiscence Characteristics from Conversation as Adaptive Features of Old Age.” International Journal of Aging and Human Development 5 (1974): 281-94.
Confucius. Liji: The Book of Rites [in Chinese]. Jinan, Shandong: Shandong Friendship Press, 2000.
Cook, Sarah, and Susie Jolly. “Unemployment, Poverty, and Gender in Urban China: Perceptions and Experiences of Laid-off Workers in Three Chinese Cities.” IDS Research Report, no. 50. Brighton, England: University of Sussex, Institute of Development Studies, 2001.
Corless, Inge B. “Hospice and Hope: An Incompatible Duo?” American Journal of Hospice and Palliative Care 9 (May/June 1992): 10-12.
Corr, Charles A., Clyde Nabe, and Donna Corr. Death and Dying, Life and Living. 4th ed. Belmont, CA: Wadsworth, 2003.
Cousins, Norman. Head First: The Biology of Hope. New York: E. P. Dutton, 1989.
Coward, Doris D. “Meaning and Purpose in the Lives of Persons with AIDS.” Public Health Nursing 11 (1994): 331-36.
Crites, Stephen D. “Narrative Quality of Experience.” Journal of the American Academy of Religion 39 (Sept. 1971): 291-311.
DeGraff, Geoffrey (a.k.a. Thanissaro Bhikkhu). “Life Isn’t Just Suffering.” http://www.thaiexotictreasures.com/suffering.html (accessed May 20, 2008).
Deng, Ming-Dao. Scholar Warrior: An Introduction to the Tao in Everyday Life. San Francisco: Harper San Francisco, 1990.
De Shazer, Steve. Putting Difference to Work. New York: W. W. Norton, 1991.
Dhammavihari, Bhikku. “Euthanasia: A Study in Relation to Original Theravaden
Thinking.” Y2000 Global Conference on Buddhism, Singapore June 3-4, 2000. http://www.metta.lk/english/euthanasia.htm (accessed May 20, 2008).
Donald, Anna. “What is Quality of Life?” In What is… ? Series. http://www.whatisseries.co.uk (accessed May 20, 2008).
Dunlop, John. “A Physician’s Advice to Spiritual Counselors of the Dying.” Trinity Journal 14, no. 2 (Fall 1993): 201-14.
Dworkin, Gerald. The Theory and Practice of Autonomy. Cambridge: Cambridge University Press, 1988.
Edlund, Matthew, and Laurence Tancredi. “Quality of Life: An Ideological Critique.” Perspectives in Biology and Medicine 28, no. 4 (Summer 1985): 591-607.
Elwell, Walter A., ed. Evangelical Dictionary of Theology. Grand Rapids, MI: Baker Book House, 1984.
Erikson, Erik H. “Human Strength and the Cycle of Generations.” Insight and Responsibility: Lectures on the Ethical Implications of Psychoanalytical Insight. New York: W. W. Norton, 1994.
________. Identity and the Life Cycle. New York: International Universities Press, 1959.
________. Identity, Youth, and Crisis. New York: W. W. Norton, 1968.
“Euthanasia: The Buddhist View.” BBC Religion and Ethics Forum. Feb. 24, 2004. http://www.bbc.co.uk/religion/religions/buddhism/buddhistethics/euthanasiasuicide.shtml (accessed May 20, 2008).
Fanslow-Brunjes, Cathleen, Patricia E. Schneider, and Lee H. Kimmel. “Hope: Offering Comfort and Support for Dying Patients.” Nursing 27, no. 3 (1997): 54-57.
Farran, Carol J., Kaye A. Herth, and Judith M. Popovich. Hope and Hopelessness: Critical Clinical Concepts. Thousand Oaks, CA: Sage Publications, 1995.
Fawzy, Fawzy I., Norman Cousins, et al. “A Structured Psychiatric Intervention for Cancer Patients. I. Changes over Time in Methods of Coping and Affective Disturbance.” Archives of General Psychiatry 47, no. 8 (1990): 720-25.
Fife, Betsy L. “The Measurement of Meaning in Illness.” Social Science Medicine 40 (1995): 1021-28.
Fisher, Walter R. “Narration as Human Communication Paradigm: The Case of Public Moral Argument.” Communication Monographs 51 (1984): 1-22.
Frankl, Viktor Emil. Man’s Search for Meaning: An Introduction to Logotherapy. Rev. and enl. ed. Trans. Ilse Lasch. Boston: Beacon Press, 1962.
________. The Unconscious God. New York: Simon and Schuster, 1975.
Freud, Sigmund. Standard Edition of the Complete Psychological Works of Sigmund Freud. 24 volumes. Eds. James Strachey et al. (London: Hogarth Press, c1966, 1974), 119-23.
Fromm, Erich. The Revolution of Hope: Toward a Humanized Technology. New York: Harper & Row, 1968.
Furman, Ben, and Tapani Ahola. Solution Talk: Hosting Therapeutic Conversations. New York: W. W. Norton, 1992.
Gardner, Richard A. Psychotherapy with Children of Divorce. New York: Jason Aronson, 1976.
Gu, Edward. “Labor Market Insecurities in China.” Geneva: International Labor Office Publ., May 2003. http://www.ilo.org/public/english/protection/ses/download/docs/ labor_china.pdf (accessed May 14, 2008).
Guignon, Charles B. The Cambridge Companion to Heidegger. 2nd ed., rev. Cambridge: Cambridge University Press, 2006.
Hauerwas, Stanley. Naming the Silences: God, Medicine, and the Problem of Suffering. Grand Rapids, MI: Eerdmans Publ., 1990.
Hegel, Georg Wilhelm Friedrich. Phenomenology of Spirit. Trans. Arnold V. Miller. Oxford: Clarendon Press, 1977.
Heidegger, Martin. Poetry, Language, Thought. Trans. Albert Hofstadter. New York: Harper & Row, 1971.
________. The Question Concerning Technology and Other Essays. Trans. William Lovitt. New York: Harper & Row, 1977.
Heschel, Abraham Joshua. The Prophets. New York: Harper & Row, 1962.
Hesketh, Therese, and Wei-xing Zhu. “Health in China: The Healthcare Market.” British Medical Journal 314 (2004): 1616-18.
Hippocrates. “Hippocratic Oath.” The National Institutes of Health. History of Medicine Division. http://www.nlm.nih.gov/hmd/greek/greek_oath.html (accessed May 20, 2008).
Hirth, Alexandra M., and Miriam J. Stewart. “Hope and Social Support as Coping Resources for Adults Waiting for Cardiac Transplantation.” Canadian Journal of Nursing Research 26, no. 3 (1994): 31-48.
Hoff, Benjamin. The Tao of Pooh. New York: E. P. Dutton, 1982.
Hoffman, Ernst. “Hope.” In Dictionary of New Testament Theology. Ed. Colin Brown. Vol. 2. Grand Rapids, MI: Zondervan, 1976.
Horn, Joshua S. Away with All Pests: An English Surgeon in People’s China: 1954-1969. New York: Monthly Review Press, 1971.
Hunter, Rodney J., et al., ed. Dictionary of Pastoral Care and Counseling. Nashville, TN: Abingdon Press, 1990.
Kahn, Joseph. “China’s ‘Haves’ Stir the ‘Have Nots’ to Violence.” New York Times, December 31, 2004, A1.
Kant, Immanuel. Critique of Pure Reason. Trans. John Miller Dow Meiklejohn. Mineola, NY: Courier Dover Publications, 2003.
Kasulis, Thomas P. Intimacy or Integrity: Philosophy and Cultural Difference. Honolulu: University of Hawai’i Press, 2002.
Kaveny, M. Cathleen. “Cultivating Hope in Troubled Times.” Lumen, University of Notre Dame, Nov. 2005. http://www.nd.edu/~lumen/2005_11/index.shtml (accessed May 25, 2008).
Keats, John. “Last Sonnet.” In The Poetical Works of John Keats, ed. H. Buxton Forman, 486. London: Oxford University Press, 1931.
Kekes, John. “The Meaning of Life.” Midwest Studies in Philosophy 24 (2000): 17-34.
Keown, Damien. “Buddhism and Suicide: The Case of Channa.” Journal of Buddhist Ethics, 3 (1996): 8-31.
Kogon, Manuela M., David Spiegel, et al. “Effects of Medical and Psychotherapeutic Treatment on the Survival of Women with Metastatic Breast Carcinoma.“ Cancer 80, no. 2 (15 July 1997): 225-30.
Kübler-Ross, Elisabeth. On Death and Dying. New York: Macmillan, 1969.
________. “Therapy with the Terminally Ill.” In Death: Current Perspectives, ed. Edwin S. Shneidman. 2nd ed. Palo Alto, CA: Mayfield Publishing, 1980.
Lao-tzu. Tao Te Ching. Trans. Dim-cheuk Lau. London: Penguin Books, 1963.
Lazarus, Richard S. “Positive Denial: The Case for Not Facing Reality.” Interview by Daniel Goleman. Psychology Today 48 (Nov. 1979): 44-60.
________. “Stress and Coping as Factors in Health and Illness.” In Psychosocial Aspects of Cancer, ed. Jerome Cohen et al. New York: Raven Press, 1982.
Lester, Andrew D. Hope in Pastoral Care and Counseling. Louisville: Westminster John Knox Press, 1995.
Leung, Thomas In-sing. From Suffering to Hope [in Chinese]. CD-ROM. Vancouver, BC: Culture Regeneration Research Society Productions Association, 2004.
Li, Chun-ling. “The Class Structure of China’s Urban Society during the Transitional Period.” Social Sciences in China 23, no. 1 (2002): 91-99.
Li, De-quan. “The Right Direction in Providing Health Care for the People” [in Chinese], lecture delivered at the First National Health Conference, Beijing, Aug. 7-19, 1950. People’s Daily Oct. 23, 1950, Editorial.http://read.woshao.com/400327 (accessed May 25, 2009).
Li, Lan-qing. “The Reforms of the Basic Health Insurance System and the Health and Medicine System for Urban Staff and Workers” [in Chinese], delivered at National Conference in Shanghai, China, July 24-26, 2000. http://www.shanghai.gov.cn/shanghai/node2314/node3124/node3125/node3127/userobject6ai269.html (accessed May 24, 2009).
Li, Pei-lin. “Problems and Trends of China’s Social and Economic Developments” [in Chinese]. http://china.com.cn/chinese/zhuanti/2004shxs/483054.htm (accessed May 14, 2008).
Lim, Meng-kin., Hui Yang, Tuo-hong Zhang, Wen Feng and Zi-jun Zhou. “Public Perceptions of Private Health Care in Socialist China.” Health Affairs 23 (2004): 222-34.
Liu, Gordon G., et al. “Equity in Health Care Access : Assessing the Urban Health Insurance Reform in China.” Social Science and Medicine 55, no. 10 (Nov. 2002): 1779-94.
Liu, Yuan-li, Ke-qin Rao, and William C. Hsiao. “China’s Public Health Care System: Facing the Challenges.” Bulletin of the World Health Organization 82 (2004): 532-38.
________. “Development of the Rural Health Insurance System in China.” Health Policy and Planning 19 (2004): 159-65.
________. “Medical Spending and Rural Impoverishment in China.” Journal of Health, Population, and Nutrition 21 (2003): 216-22.
Liu, Zhong-xiang. “A Study of the Problem Related to Medical Assistance for Urban Poor.” Table 2. Sociology Department, People’s University of China, 2003.
Lo, Ping-cheung. “Confucian Values of Life and Death and Euthanasia.” Annual of the Society of Christian Ethics, 19 (1999): 313-33.
Loder, James E. The Transforming Moment: Understanding Convictional Experiences. San Francisco: Harper & Row, 1981.
Lynch, William F. Images of Hope: Imagination as Healer of the Hopeless. Baltimore: Helicon, 1965.
Macmurray, John. Persons in Relation. London: Faber & Faber, 1961.
Macquarrie, John. Christian Hope. New York: Seabury Press, 1978.
________ In Search of Humanity. New York: Crossroad, 1983.
________“Pilgrimage in Theology.” Epworth Review 7, no. 1 (Jan. 1980): 47-52.
Marcel, Gabriel. “Despair and the Object of Hope.” In The Sources of Hope, ed. Ross Fitzgerald, 44-66. Trans. Jean Nowotny. Rushcutters Bay, Australia; Elmsford, NY: Pergamon Press, 1979.
________. Homo Viator: Introduction to a Metaphysic of Hope. Gloucester, MA: Peter Smith, 1978.
Marshall, Ellen Ott. Though the Fig Tree Does Not Blossom: Toward a Responsible Theology of Christian Hope. Nashville: Abingdon Press, 2006.
Massie, Mary Jane, et al. “Depression and Suicide in Patients with Cancer.” Journal of Pain and Symptom Management 9 (1994): 325-40.
May, Rollo. Freedom and Destiny. New York: W. W. Norton, 1981.
________. Love and Will. New York: W. W. Norton, 1969.
McMahon, Arthur W., and Paul J. Hudick. “Reminiscing: Adaptational Significance in the Aged.” Archives of General Psychiatry 10 (1964): 292-98.
Meissner, William W. Psychoanalysis and Religious Experience. New Haven: Yale University Press, 1984.
Mencius. Mencius, trans. D.C. Lau. Harmondsworth: Penguin, 1970.
Metz, Johannes B. Faith in History and Society: Toward a Practical Fundamental Theology. Trans. David Smith. New York: Seabury Press, 1980.
Mijuskovic, Ben. Loneliness in Philosophy, Psychology, and Literature. Assen, Netherlands: Van Gorcum, 1979.
Minear, Paul S. Christian Hope and the Second Coming. Philadelphia: Westminster Press, 1954.
Mishel, Merle H. “The Theory of Uncertainty in Illness.” Image 20, no. 4 (1988): 225-32.
Mitchell, Deborah R. “The ‘Good’ Death: Three Promises to Make at the Bedside.” Geriatrics 52, no. 8 (1997): 591-92.
Moltmann, Jürgen. In the End, the Beginning: The Life of Hope. Trans. Margaret Kohl. Minneapolis, MN: Fortress Press, 2004.
________. Theology of Hope; On the Ground and the Implications of a Christian Eschatology. Trans. James W. Leitch. New York: Harper & Row, 1975.
Moyers, Bill D., Betty S. Flowers, and David Grubin. Healing and the Mind. New York: Doubleday, 1993.
Nichols, Aidan. The Art of God Incarnate : Theology and Image in Christian Tradition. London: Darton, Longman and Todd, 1980.
Nietzsche, Friedrich. The Birth of Tragedy. Trans. Walter Kaufmann. New York: Vintage Press, 1966.
________. The Birth of Tragedy and the Genealogy of Morals. Trans. Francis Golffing. New York: Doubleday, 1956.
________. The Gay Science. Trans. Walter Kaufmann. New York: Vintage Books, 1974.
________. On the Genealogy of Morals. Trans. Walter Kaufmann and R. J. Hollingdale. New York: Vintage Press, 1967.
________. Thus Spake Zarathustra. Trans. Thomas Common. New York: Heritage Press, 1967.
________. “Twilight of the Idols.” In The Portable Nietzsche, trans. and ed. Walter Kaufmann, 463-564. New York: Penguin, 1976.
________. The Will to Power. Trans. Walter Kaufmann and R. J. Hollingdale. Ed. Walter Kaufmann. New York: Vintage Press, 1968.
Nouwen, Henri J.M. Out of Solitude:Three Meditations on the Christian Life. Notre Dame, IN: Ave Maria Press, 1974.
Ogden, Schubert. “The Meaning of Christian Hope.” Union Seminary Quarterly Review 30 (Winter-Summer 1975): 153-64.
Ou, Ai-hua, and Yan Zhu. “Analysis of Condition of Elderly People and Their Health Service Utilization in Guiyang City.” Chinese Primary Health Care 14, no. 3 (2000): 47-48.
Pannenberg, Wolfhart. Anthropology in Theological Perspective. Trans. Matthew J. O’Connell. Philadelphia: Westminster Press, 1985.
________. Theology and the Kingdom of God. Ed. Richard J. Neuhaus. Philadelphia: Westminster Press, 1969.
Parker-Oliver, Deborah. “Redefining Hope for the Terminally Ill.” American Journal of Hospice and Palliative Care 19, no. 2 (2002): 115-20.
________. “The Social Construction of a Dying Role: The Hospice Drama.” Omega – Journal of Death and Dying 40, no. 4 (2000): 19-38.
Pattison, E. Mansell. “The Experience of Dying.” American Journal of Psychotherapy 21 (1967): 32-43.
People’s Republic of China.Bureau of Statistics. China Statistical Yearbook. Beijing: China Statistics Press, 1998, 2001.
________. Gansu Province Department of Health. “History and Development of Health Care System in Gansu Province.” Gansu, 2000.
________. Ministry of Health. Annual Report, 2001. Beijing, 2001.
________. Ministry of Health, Ministry of Finance, and Ministry of Agriculture. The Circular Concerning the Establishment of a New-Style Rural Cooperative Health Care System. Beijing, Jan. 10, 2003.
________. Ministry of Labor and Social Security. “An Investigative and Analytical Report on the Reform of the Health Insurance System in Zhenjiang, Changshu, and Shanghai” [in Chinese]. Beijing: Social Security Research Institute Publ., Nov. 11, 2001.
________. “New Rural Medical Care System to Insure Farmers’ Health,” March 30, 2006. http://www.china-embassy.org/eng/xw/t243199.htm (accessed May 14, 2008).
________. Social Security Department. Report on Reform of Health Care System for Staff and Workers [in Chinese]. Beijing: Gaige, 1996.
Plato. The Republic. Introd. Charles M. Bakewell. New York: Charles Scribner, 1928.
________. Plato’s Phaedrus. Trans. Reginald M. Hackforth. London: Cambridge University Press, 1952.
Progoff, Ira. The Dynamics of Hope: Perspectives of Process in Anxiety and Creativity, Imagery and Dreams. New York: Dialogue House Library, 1985.
Pruyser, Paul W. “Phenomenology and Dynamics of Hoping.” Journal for the Scientific Study of Religion 3 (1964): 86-96.
________. Between Belief and Unbelief. New York: Harper & Row, 1974.
________. The Play of the Imagination: Toward a Psychoanalysis of Culture. New York: International Universities Press, 1983.
________“Maintaining Hope in Adversity.” Pastoral Psychology 35 (1986): 120-31.
Qin, Yan. “Schiavo’s Fate Fires Debate on Euthanasia.” China Daily, Mar. 23, 2005, http://www.chinadaily.com.cn/english/doc/2005-03/23/content_427546.htm (accessible May 14, 2008).
Ratner, Carl, and Lu-mei Hui. “Theoretical and Methodological Problems in Cross-Cultural Psychology.” Journal for the Theory of Social Behaviour 33, no. 1 (2003): 67-94.
Reese, Dona J., and Dean R. Brown. “Psychosocial and Spiritual Care in Hospice: Differences between Nursing, Social Work, and Clergy.” Hospice Journal 12, no.1 (1997): 29-41.
Remen, Rachel Naomi. A quote from Healing and The Mind by Bill D. Moyers, Betty S. Flowers, and David Grubin (New York: Doubleday, 1993), 357. Publication information for Rachel Remen not provided.
Richards, Victor. “Death and Cancer.” In Death: Current Perspectives, ed. Edwin S. Shneidman, 322-30. Palo Alto, CA: Mayfield Publishing, 1980.
Richardson, Robert L. “Where There is Hope, There is Life: Toward a Biology of Hope.” Journal of Pastoral Care 54, no. 1 (Spring 2000): 75-83.
Rideout, Elizabeth, and Maureen Montemuro. “Hope, Morale and Adaptation in Patients with Chronic Heart Failure.” Journal of Advanced Nursing 11 (1986): 429-38.
Rogers, James. The Dictionary of Cliches. New York: Ballantine Books, 1985.
Salmond, S. D. F. Christian Doctrine of Immortality. 3rd ed. Edinburgh: T. & T. Clark, 1897.
Sarbin, Theodore R. “The Narrative as a Root Metaphor for Psychology.” In Narrative Psychology: The Storied Nature of Human Conduct, ed. Theodore R. Sarbin, 3-21. New York: Praeger, 1986.
Sartre, Jean-Paul. Being and Nothingness: An Essay in Phenomenological Ontology. Trans. Hazel E. Barnes. New York: Citadel Press 1956.
Scarry, Elaine. The Body in Pain: The Making and Unmaking of the World. New York: Oxford University Press, 1985.
Schopenhauer, Arthur. The World as Will and Representation. Trans. E. F. J. Payne. Vol. 2. Indian Hills, CO: Falcon’s Wing Press, 1958.
________. Parerga and Paralipomena: Short Philosophical Essays. Trans. E.F.J. Payne. 2 vols. Oxford: Clarendon Press, 1974.
Scott, W. Clifford M. “Depression, Confusion, and Multivalence.” International Journal of Psychoanalysis 41 (1960): 497-503.
Shorr, Joseph E., Gail E. Sobel, et al., eds. Imagery: Its Many Dimensions and Applications. New York: Plenum, 1980.
Smith, David L. A Handbook of Contemporary Theology. Wheaton, IL: Victor Books, 1992.
Smith, Douglas C., and Michael F. Maher. “Achieving a Healthy Death: The Dying Person’s Attitudinal Contributions.” Hospice Journal 9 (1993): 21-32.
Smith, Stephen M. “Hope, Theology of.” In Evangelical Dictionary of Theology, ed. Walter A. Elwell, 577-79. 2nd ed. Grand Rapids, MI: Baker Book House, 2001.
Snook, Lee E. “Death and Hope – An Essay in Process Theology.” Dialog 15, no. 2 (Spring 1976): 123-30.
Snyder, Charles R. The Psychology of Hope: You Can Get There From Here. New York: Free Press, 1994.
________, and Shane J. Lopez, eds. Handbook of Positive Psychology. Oxford: Oxford University Press, 2002.
Solomon, William David. “Double Effect.” In The Encyclopedia of Ethics, 2nd ed., eds. Lawrence C. Becker and Charlotte B. Becker, 418-20. Florence, KY: Routledge Press, 2001.
Song, Xiao-wu, and Hao Liu. “The Reform of the Health Insurance System Accompanying Measures.” In Report on the Reform and Development of China’s Social Security System [in Chinese], ed. Xiao-wu Song. Beijing: Renmin University of China Press, 2001.
Sorajjakool, Siroj, and Henry Lamberton, eds. Spirituality, Health, and Wholeness: An Introductory Guide for Health Care Professionals. New York: Haworth Press, 2004.
Spiegel, David, and Irvin D. Yalom. “A Support Group for Dying Patients.” International Journal of Group Psychotherapy 28, no. 2 (1978): 233-45.
________, et al. “The Effect of Psychosocial Intervention on Survival of Patients with Metastatic Breast Cancer.” The Lancet 2 (14 Oct. 1989): 888-91.
Stone, Howard W., ed. Strategies for Brief Pastoral Counseling.Minneapolis, MN: Fortress Press, 2001.
Tada, Joni E. When Is It Right to Die? Suicide, Euthanasia, Suffering, Mercy. Grand Rapids, MI: Zondervan Publishing House, 1992.
Thomas Aquinas. Summa Theologica. Vol. 2. Trans. Wilfrid Lescher. London: Thomas Baker, 1906.
Tillich, Paul. “The Right to Hope: A Sermon.” Christian Century 107, no 33 (Nov. 14, 1990): 1064-67.
Triandis, Harry C. Culture and Social Behavior. New York: McGraw-Hill, 1994.
Tse, Chun-yan, Alice Chong, and Janet Sui-yee Fok. “Breaking Bad News: A Chinese Perspective.” Palliative Medicine 17 (2003): 339-43.
Tu, Wei-ming. Confucian Thought: Selfhood as Creative Transformation. Albany: State University of New York Press, 1985.
Unamuno, Miguel de. The Tragic Sense of Life. Trans. J. E. Crawford Flitch. New York: Cosimo Classics, 2005.
Waley, Arthur, trans. The Analectsof Confucius. New York: Everyman’s Library, 2001.
Wang, Dong-jin. “The Importance and Urgency of Sufficiently Understanding the Reform of the Health Insurance System for Urban Staff and Workers” [in Chinese]. China Labor 158 (Jan 1999): 4-7.
________ed. The Reform and Development of China’s Social Security System [in Chinese]. Beijing: Falu Press, 2001.
Wang, Mei-Ling, Shuo Zhang, and Xiao-Wan Wang. WTO, Globalization, and China’s Health Care System. New York: Palgrave Macmillan, 2007.
Weisman, Avery D. On Dying and Denying: A Psychiatric Study of Terminality. New York: Behavioral Publications, 1972.
Wells, Richard A. Planned Short-Term Treatment. New York: Free Press, 1982.
Wernow, Jerome R. “Saying the Unsaid: Voicing Quality-of-Life Criteria in an Evangelical Sanctity-of-Life Principle.” Journal of the Evangelical Theological Society 391, no. 1 (March 1996): 103-22.
Wholihan, Dorothy. “The Value of Reminiscence in Hospice Care.” American Journal of Hospice Palliative Care 9 (1992): 33-35.
Williams, Alan. “’Need’ – an Economic Exegesis.” In The Economics of Health, ed. Anthony J. Culyer, 259-72. Vol. 1. Brookfield, VT: Edward Elgar Pub., 1991.
Winnicott, Donald W. “Transitional Objects and Transitional Phenomena.” In Collected Papers: Through Paediatrics to Psycho-Analysis. New York: Basic Books, 1958.
Wong, Chack-kie, Vai Io Lo, and Kwong-leung Tang. China’s Urban Health Care Reform: From State Protection to Individual Responsibility. Lanham, MD: Lexington Books, 2006.
Wong, David B. “Pluralistic Relativism.” In Moral Concepts, eds. Peter A. French, Theodore E. Uehling, Jr., and Howard K. Wettstein, 378-99. Notre Dame, IN: University of Notre Dame Press, 1996.
________. “Comparative Philosophy – Chinese and Western.” Rev. 2005. Stanford Encyclopedia of Philosophy. http://plato.stanford.edu/entries/comparphil-chiwes (accessed May 20, 2008).
Wong, Paul T. P. “Chinese Positive Psychology.” In Encyclopedia of Positive Psychology, ed. Shane Lopez, 148-56. Malden, MA: Wiley-Blackwell Pub., 2009.
________. “The Wisdom of Positive Acceptance.” President’s Column, International Network on Personal Meaning, 2004. http://www.meaning.ca/archives/presidents_columns/pres_col_feb_2004_ positive-acceptance.htm (accessed May 20, 2008).
________ and Catherine Stiller. “Living with Dignity and Palliative Care.” In End of Life Issues: Interdisciplinary and Multidimensional Perspectives, ed. Brian de Vries, 77-94. New York: Springer, 1999.
World Bank. China: National Development and Sub-National Finance: A Review of Provincial Expenditures. Report No. 22951-CHA. Washington, DC: World Bank, 2002.
Xiong, Yue-gen. “Social Policy for the Elderly in the Context of Aging in China: Issues and Challenges of Social Work Education.” International Journal of Welfare for the Aged 1 (1999): 107-22.
Yalom, Irvin D. Existential Psychotherapy. New York: Basic Books, 1980.
________. The Theory and Practice of Group Psychotherapy. 4th ed. New York: Basic Books, 1995.
Yardley, Jim. “Rural Exodus for Work Fractures Chinese Family.” New York Times, Dec. 21, 2004, A1.
________“Xin-min Village Journal: A Deadly Fever, Once Defeated, Lurks in a Chinese Lake.” New York Times, Feb. 22, 2005, A4.
Young, Julian. The Death of God and the Meaning of Life. London: Routledge, 2003.
Zhou, Li-ping and Rui-zi Wang. “Analysis of Health Need and Utilization of Elderly Population in Hangzhou City” [in Chinese]. Journal of Zhejiang Medical University 27, no. 2 (1998): 84-87.
Zhuan, Hui-lin. “Urban Deprived Groups in the New Era: Studying the Construction of a Health Care Protection Mechanism” [in Chinese]. Market and Population Analysis. May 23, 2003.
Zimmerli, Walther. Old Testament Theology in Outline. Trans. David E. Green. Atlanta: John Knox Press, 1978.
END OF BOOK – HOPE YOU HAVE FOUND IT HELPFUL